- 1Department of Psychology, Faculty of Medicine and Psychology, Sapienza University of Rome, Rome, Italy
1羅馬第一大學醫學與心理學繫心理學系,義大利羅馬 - 2Primary Care Unit, Department of Public Health and Primary Care, University of Cambridge, Cambridge, United Kingdom
2劍橋大學公共衛生與初級保健系初級保健單位,英國劍橋 - 3Sleep and Circadian Neuroscience Institute, Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, United Kingdom
3睡眠與晝夜節律神經科學研究所,牛津大學納菲爾德臨床神經科學系,英國牛津
Background: Executive functions (EFs) are involved in the control of basic psychological processes such as attention and memory and also contribute to emotion regulation. Research on the presence of EFs impairments in insomnia yielded inconsistent results. Therefore, we performed a systematic review of the literature on three EFs: inhibitory control, working memory, and cognitive flexibility in adults with insomnia in order to investigate the presence and magnitude of insomnia-related EFs impairments.
背景:執行功能(EF)涉及注意力和記憶等基本心理過程的控制,也有助於情緒調節。關於失眠中 EF 損傷的研究得出了不一致的結果。因此,我們對成人失眠患者的抑制控制、工作記憶和認知靈活性這三種 EF 的文獻進行了系統性回顧,以調查與失眠相關的 EF 損傷的存在和嚴重程度。
Methods: PubMed, Scopus, Medline, and PsycINFO were searched. Risk of bias assessment of included studies was performed by two independent researchers. Findings were summarised using both a narrative approach and meta-analysis. Cohen's d was calculated at 95% confidence interval (CI) as effect size of between groups differences.
方法:檢索 PubMed、Scopus、Medline 和 PsycINFO。納入研究的偏倚風險評估由兩位獨立研究人員進行。使用敘述方法和薈萃分析總結了研究結果。 Cohen's d以 95% 信賴區間 (CI) 計算,作為組間差異的效果量。
Results: Twenty-eight studies comparing adult individuals with a diagnosis of insomnia and healthy controls on neuropsychological measures of EFs were included. Narrative synthesis revealed substantial variability across study findings. Factors that were primarily hypothesised to account for this variability are: objective sleep impairments and test sensitivity. Exploratory meta-analysis showed impaired performance of small to moderate magnitude in individuals with insomnia as compared to controls in reaction times, but not accuracy rates, of inhibitory control (d = −0.32, 95% CI: −0.52 to −0.13) and cognitive flexibility tasks (d = −0.30, 95% CI: −0.59 to −0.01). Performance in working memory tasks was also significantly impacted (d = −0.19, 95% CI: −0.38 to −0.00). Effects sizes were larger when insomnia was associated with objective sleep impairments, rather than normal sleep.
結果:納入了 28 項研究,比較了診斷為失眠的成年人和健康對照組對 EF 神經心理測量的影響。敘事綜合揭示了研究結果的巨大差異。主要假設解釋這種變異性的因素是:客觀睡眠障礙和測試敏感性。探索性統合分析顯示,與對照組相比,失眠個體的抑制控制( d = -0.32,95% CI:-0.52 至-0.13)和認知的反應時間(但準確率)有小到中度的受損。工作記憶任務的表現也受到顯著影響( d = -0.19,95% CI:-0.38 至 -0.00)。當失眠與客觀睡眠障礙而不是正常睡眠相關時,效果更大。
Conclusions: We gathered evidence supporting small to moderate deficits in EFs in individuals with insomnia. Due to the small sample size results should be considered preliminary and interpreted carefully.
結論:我們收集的證據支持失眠個體存在小到中度的 EF 缺陷。由於樣本量較小,應初步考慮結果並仔細解釋。
Introduction 介紹
Rationale 基本原理
Insomnia disorder is defined by difficulty falling asleep, maintaining sleep or early morning awakenings (American Psychiatric Association, 2013). Concomitant daytime consequences such as fatigue, reduction in motivation and energy, mood instability, and cognitive impairments are crucial components of insomnia (Shekleton et al., 2010). Symptoms should present at least three times a week over a period of 3 months to meet the diagnostic criteria for insomnia (American Psychiatric Association, 2013). Epidemiological data estimate the prevalence of insomnia disorder from 6 to 20% in industrialised societies, with rates varying depending on country under study and methodological quality (Calem et al., 2012; Chaput et al., 2018).
失眠症的定義是難以入睡、維持睡眠或清晨醒來(美國精神醫學會,2013 )。隨之而來的白天後果,如疲勞、動力和精力下降、情緒不穩定和認知障礙,是失眠的重要組成部分( Shekleton 等,2010 )。症狀應在 3 個月內每週至少出現 3 次,才能滿足失眠的診斷標準(美國精神醫學會,2013 年)。流行病學數據估計,工業化社會中失眠症的盛行率為 6% 至 20%,具體比例因研究國家和方法品質而異( Calem 等,2012 ; Chaput 等,2018 )。
Deficits in the control of cognitive and emotional processes are key characteristics of insomnia, as highlighted by influential models on the disorder (Perlis et al., 1997; Harvey, 2002; Espie et al., 2006). For instance, according to Harvey (2002), patients with insomnia are unable to exert control over night-time intrusive cognitions and engage in diurnal repetitive and unwanted thoughts, such as ruminations, i.e., passively and repetitively focusing on the consequences of insomnia. Impairments in the domain of concentration, memory, attention, and emotion regulation are also generally reported in this population (Kyle et al., 2013; Harris et al., 2015; Cellini, 2016). Taken together, these findings raise the question of whether executive functions (EFs), the higher order cognitive processes which exert top-down control over basic psychological functions like attention, memory, and contribute to emotion regulation (Diamond, 2013; Yang et al., 2016), are also impacted in insomnia. To answer this question, we aimed to conduct a systematic review and exploratory meta-analysis of the literature examining EFs in insomnia disorder in an adult population. Before introducing our study, we discuss conceptual models of EFs, their clinical correlates and the role of EFs in insomnia.
認知和情緒過程的控制缺陷是失眠的關鍵特徵,有關疾病的有影響力的模型強調了這一點( Perlis 等,1997 ; Harvey,2002 ; Espie 等,2006 )。例如,根據Harvey (2002)的研究,失眠患者無法控制夜間侵入性認知,並會在白天進行重複性和不必要的想法,例如沉思,即被動地、反覆地關注失眠的後果。據報導,該族群普遍存在註意力、記憶力、注意力和情緒調節方面的障礙( Kyle et al., 2013 ; Harris et al., 2015 ; Cellini, 2016 )。總而言之,這些發現提出了這樣一個問題:執行功能(EF),即對注意力、記憶等基本心理功能進行自上而下的控制的高階認知過程,是否有助於情緒調節( Diamond,2013 ; Yang等人,2013)。為了回答這個問題,我們的目的是對成人失眠 EF 的文獻進行系統性回顧和探索性統合分析。在介紹我們的研究之前,我們先討論 EF 的概念模型、它們的臨床相關性以及 EF 在失眠中的作用。
EFs are considered top-down, higher-order cognitive processes needed to control and coordinate lower-level mental processes such as memory encoding and retrieval, orienting attention, and emotion regulation, which together enable self-regulation and contribute to goal-directed behaviour (Diamond, 2013; Snyder et al., 2015). Neuropsychological and neuroimaging studies in clinical and healthy populations suggest that the prefrontal cortex (PFC) as well as parietal and cerebellar networks subserve EFs (Nowrangi et al., 2014; Yuan and Raz, 2014). However, the definition and conceptualisation of EFs remains inconsistent in the literature. Indeed, there is a lack of agreement regarding whether EFs should be considered unitarily (e.g., Duncan, 2010) or as a number of different and independent cognitive processes (e.g., Miyake et al., 2000). Moreover, conceptualisation and definition of EFs varies substantially depending on the field of study and the population of interest. This is reflected by the prevalent use of the term EFs in neuropsychology (aimed at the assessment of patients) and the term control processes in the cognitive sciences (typically aimed at investigating in healthy populations the cognitive mechanisms underlying the EFs). Given the clinical nature of this review, we use the terms EFs throughout the text.
EF 被認為是自上而下的高階認知過程,需要控制和協調較低層次的心理過程,例如記憶編碼和檢索、定向注意力和情緒調節,這些過程共同實現自我調節並有助於目標導向的行為。對臨床和健康人群的神經心理學和神經影像學研究表明,前額葉皮質 (PFC) 以及頂葉和小腦網絡有助於 EF( Nowrangi 等,2014 ; Yuan 和 Raz,2014 )。然而,文獻中 EF 的定義和概念仍然不一致。事實上,對於 EF 是否應該被單一地考慮(例如, Duncan,2010 )還是作為許多不同且獨立的認知過程(例如, Miyake 等人,2000 ),缺乏共識。此外,EF 的概念和定義根據研究領域和感興趣的人群而有很大差異。這反映在神經心理學中術語 EF(旨在評估患者)和認知科學中術語控制過程(通常旨在研究健康人群中 EF 背後的認知機制)。鑑於本次綜述的臨床性質,我們在全文中使用術語 EF。
Different conceptualisations and classifications of EFs have been developed over several decades (see Gratton et al., 2017 for a review). Recently, an influential model hypothesised that the performance on complex EF tasks is underpinned by three core EFs: inhibitory control, working memory, and cognitive flexibility (Miyake et al., 2000; Diamond, 2013). Inhibitory control refers to the ability to reduce the effect of strong internal predispositions, automatic schemata or responses when they are not useful for accomplishing the task goal. Inhibitory control is therefore needed to suppress thoughts, emotions, motor responses and irrelevant stimuli (Aron et al., 2004). Working memory involves the ability to hold and manipulate goal-related information in mind (Repovs and Baddeley, 2006). Finally, cognitive flexibility refers to the ability to readily change perspective, demands or priorities, and to quickly adjust from set-shifting (Miyake et al., 2000). Given its wide use in cognitive and clinical literature, we decided to focus the present systematic review on the tripartite model of EFs, based on inhibitory control, working memory, and cognitive flexibility. This tripartite model of EFs also overlaps with the model of “executive control” adopted in insomnia research by Vgontzas et al. (2013) in their attempt to identify different phenotypes of insomnia from symptom severity and biological correlates, as further described below.
幾十年來,不同的 EF 概念和分類得到了發展(參見Gratton 等人,2017 年的綜述)。最近,一個有影響力的模型假設複雜 EF 任務的表現由三個核心 EF 支撐:抑制控制、工作記憶和認知靈活性( Miyake 等,2000 ; Diamond,2013 )。抑制控制是指當強烈的內在傾向、自動圖式或反應對完成任務目標無用時,減少它們的影響的能力。因此,需要抑制性控制來抑制思想、情緒、運動反應和無關的刺激( Aron 等,2004 )。工作記憶涉及在頭腦中保存和操縱與目標相關的資訊的能力( Repovs 和 Baddeley,2006 )。最後,認知彈性是指能夠輕鬆改變觀點、需求或優先事項,並從設定轉移中快速調整的能力( Miyake et al., 2000 )。鑑於其在認知和臨床文獻中的廣泛應用,我們決定將目前的系統性綜述集中在基於抑制控制、工作記憶和認知靈活性的 EF 三方模型上。這種EF的三方模型也與Vgontzas等人在失眠研究中所採用的「執行控制」模式有重疊。 (2013)他們試圖根據症狀嚴重程度和生物學相關性來識別失眠的不同表型,如下文進一步所述。
Although individuals with insomnia commonly report subjective difficulties in different cognitive functions involving executive control like attention, memory, and concentration (Kyle et al., 2013; Harris et al., 2015; Cellini, 2016), objective EFs deficits have been difficult to capture through standardised measures in laboratory settings. Additionally, few reviews on EFs in insomnia have been published to date. A review on daytime impairments in insomnia concluded that on tests of attentional shifting and working memory, individuals with insomnia generally perform worse than good sleepers (Shekleton et al., 2010). However, the authors did not include these tests within the EFs domain and instead included planning, reasoning, flexibility, and multitasking in this category. Performance on these EFs were mostly preserved in individuals with insomnia.
儘管失眠患者通常報告在涉及執行控制(如注意力、記憶力和注意力)的不同認知功能方面存在主觀困難( Kyle 等,2013 ; Harris 等,2015 ; Cellini,2016 ),但客觀EF 缺陷很難捕捉通過實驗室環境中的標準化措施。此外,迄今為止,關於 EF 治療失眠的評論還很少。對失眠造成的白天損害的回顧得出結論,在註意力轉移和工作記憶測試中,失眠者的表現通常比睡眠品質好的人差( Shekleton 等,2010 )。然而,作者並沒有將這些測驗納入 EF 領域,而是將計畫、推理、靈活性和多工處理納入這個類別。失眠患者在這些 EF 上的表現大多保持不變。
Recent evidence suggests relevant clinical correlates of EFs impairments that may be of particular interest for insomnia research. For instance, EFs have been associated with poor cognitive self-regulatory strategies, including rumination. A recent meta-analysis of correlational studies showed that poorer inhibitory control and cognitive flexibility were significantly associated with higher rumination in the general population (Yang et al., 2016). This finding may be particularly relevant for insomnia, as most theoretical models suggest a role of repetitive negative thinking such as rumination and the implementation of thought control strategies in the maintenance of the disorder (e.g., Harvey, 2002). In line with this, we recently found that rumination about symptoms of insomnia was associated with poor EFs in a clinical sample (Ballesio et al., 2018). Additionally, poor EFs have been associated with significant impairment in instrumental activities of daily living (Vaughan and Giovanello, 2010), which may contribute to lower quality of life in insomnia patients (Kyle et al., 2013) and increase indirect costs associated with insomnia (e.g., due to errors in workplace; Gustavsson et al., 2011). These potential clinical correlates of EFs in insomnia are therefore further grounds to systematically review the literature on EFs in this population.
最近的證據表明 EF 損傷的相關臨床相關性可能對失眠研究特別感興趣。例如,EF 與不良的認知自我調節策略(包括沉思)有關。最近一項相關研究的統合分析表明,一般人群中較差的抑制控制和認知靈活性與較高的沉思量顯著相關( Yang et al., 2016 )。這項發現可能與失眠特別相關,因為大多數理論模型表明重複的負面思維(例如沉思)和思想控制策略的實施在疾病的維持中發揮作用(例如, Harvey,2002 )。與此一致的是,我們最近在臨床樣本中發現,對失眠症狀的沉思與較差的 EF 相關( Ballesio 等,2018 )。此外,較差的EF與日常生活工具性活動的顯著損害有關( Vaughan和Giovanello,2010 ),這可能導致失眠患者的生活品質降低( Kyle等,2013 )並增加與失眠相關的間接成本(例如,由於工作場所的錯誤; Gustavsson 等人,2011 )。因此,EF 與失眠的這些潛在臨床相關性為系統性回顧該族群 EF 的文獻奠定了進一步的基礎。
To date, only one meta-analysis has investigated executive performance in insomnia (Fortier-Brochu et al., 2012). This included cross-sectional studies investigating daytime cognitive performance in adults with insomnia and good sleepers and published up to 2009. Findings showed that individuals with insomnia perform significantly worse than controls on tasks measuring manipulation and retention of information in working memory, with effect sizes of medium magnitude (d = 0.42). Small and non-significant effects were found with respect to tasks assessing inhibitory control (d = 0.19) and cognitive flexibility (d = 0.16). However, 6 years have passed since Fortier-Brochu et al.'s (2012) systematic review and meta-analysis on cognitive functions in insomnia, raising the need to appraise and summarise the state of the evidence again.
迄今為止,只有一項薈萃分析調查了失眠時的執行表現( Fortier-Brochu 等,2012 )。其中包括截至2009 年發表的橫斷面研究,該研究調查了失眠和睡眠良好的成年人的日間認知表現。表現明顯差於對照組,其效果量為中等震級( d = 0.42)。對於評估抑制控制( d = 0.19)和認知靈活性( d = 0.16)的任務,發現了較小且不顯著的影響。然而,自從Fortier-Brochu 等人 (2012)對失眠認知功能進行系統性回顧和統合分析以來,已經過去了 6 年,需要再次評估和總結證據狀態。
Among the factors that were previously hypothesised to account for variability between studies' findings, objective sleep received particular attention. In a large population-based study, Fernandez-Mendoza et al. (2010) concluded that only individuals with insomnia with objective short sleep duration, measured through polysomnographic records, showed impairments in executive control tasks. A subsequent theoretical review suggested that impairments in higher order cognitive processes in insomnia may be present only when the disorder is associated with shortened sleep duration (Vgontzas et al., 2013). This hypothesis may partly explain the inconsistency found in previous research on EFs. Nevertheless, it has never been tested in a systematic search of the literature. Other factors have been hypothesised to account for variability in previous results. For instance, it has been suggested that individuals with insomnia may engage increased cognitive effort in high cognitive load tasks to compensate for their deficits (Schmidt et al., 2014). Moreover, “time of the day” has been considered a confounding factor, since it is possible that individuals with insomnia and good sleeper controls have different underlying circadian rhythms, and by extension differentially affecting patterns of cognitive performance (see Shekleton et al., 2010 for a review).
在先前假設的解釋研究結果之間差異的因素中,客觀睡眠受到特別關注。在一項基於人口的大型研究中,費爾南德斯-門多薩等人。 (2010)的結論是,只有透過多導睡眠圖記錄測量的客觀睡眠時間短的失眠個體才會表現出執行控制任務的障礙。隨後的理論回顧表明,只有當疾病與睡眠時間縮短相關時,失眠中的高階認知過程損傷才可能出現( Vgontzas 等,2013 )。這個假設可以部分解釋先前 EF 研究中發現的不一致之處。然而,它從未在系統性的文獻檢索中被檢驗。也假設了其他因素來解釋先前結果的變異性。例如,有人建議,失眠者可能會在高認知負荷任務中投入更多的認知努力,以彌補他們的缺陷( Schmidt et al., 2014 )。此外,「一天中的時間」被認為是一個混雜因素,因為失眠和睡眠控制良好的個體可能具有不同的潛在晝夜節律,並且透過擴展對認知表現模式產生不同的影響(參見Shekleton 等,2010)進行審查)。
Objective 客觀的
To conduct a systematic review of the literature on inhibitory control, working memory, and cognitive flexibility in individuals with insomnia.
對失眠個體的抑制控制、工作記憶和認知靈活性的文獻進行系統性回顧。
Research Questions 研究問題
1) Are inhibitory controls, working memory, and cognitive flexibility impacted in individuals with a diagnosis of insomnia disorder?
1) 被診斷為失眠的個體的抑制控制、工作記憶和認知彈性是否受到影響?
2) Is there a relationship between objective sleep and EFs deficits in insomnia disorder?
2) 失眠的客觀睡眠與 EF 缺陷之間是否有關係?
Methods 方法
Study Design 研究設計
This study was conducted according to the preferred reporting items for systematic review and meta-analysis (PRISMA) guidelines (Moher et al., 2009) (see the PRISMA Checklist reported in Document S1).
本研究是根據系統性回顧和薈萃分析(PRISMA)指南的首選報告項目( Moher等人,2009 年)進行的(請參閱文件S1中報告的PRISMA清單)。
Participants, Interventions, Comparators
參與者、介入措施、比較者
The following inclusion criteria were applied to identified records: (1) presence of a group of adult individuals with clinical insomnia, (2) presence of a control group, (3) presence of at least one neuropsychological test assessing inhibitory control and/or working memory and/or cognitive flexibility. Given that EFs may be affected by psychoactive substances (Killgore et al., 2009, 2014), studies which allowed participants to take psychoactive medication, as well as caffeine and/or alcohol were excluded. Moreover, given that comorbid disorders may similarly affect EFs (Snyder et al., 2015), studies conducted on insomnia-comorbid samples were excluded. Studies dealing with sleep-related attentional bias were not included, as they have been recently systematically reviewed elsewhere (Harris et al., 2015). Additionally, only studies providing data to compute effect sizes were included in the meta-analytic calculations.
以下納入標準適用於確定的記錄:(1) 存在一組患有臨床失眠的成年個體,(2) 存在對照組,(3) 存在至少一項評估抑制控制和/或工作的神經心理學測試記憶和/或認知靈活性。鑑於 EF 可能受到精神活性物質的影響( Killgore 等人,2009 年, 2014 年),允許參與者服用精神活性藥物以及咖啡因和/或酒精的研究被排除在外。此外,鑑於共病可能類似地影響 EF( Snyder 等,2015 ),因此排除了對失眠共病樣本進行的研究。涉及睡眠相關注意力偏差的研究未包括在內,因為最近在其他地方對這些研究進行了系統性回顧( Harris 等人,2015 )。此外,只有提供資料來計算效應大小的研究才包含在薈萃分析計算中。
Search Strategy 搜尋策略
The literature search was performed by the first author using two strategies. First, PubMed, Scopus, Medline, and PsycINFO were searched from inception to 10th August 2018 using the following keywords: “insomnia” or “sleep disturbance” and “executive function*” or “inhibition” or “inhibitory control” or “working memory” or “flexibility.” Second, the reference lists of relevant review articles were searched. When titles of studies appeared relevant to the present review, abstracts and full-texts were screened against the eligibility criteria by the first author.
第一作者使用兩種策略進行文獻檢索。首先,從創建到2018 年8 月10 日,使用以下關鍵字對PubMed、Scopus、Medline 和PsycINFO 進行了搜尋:「失眠」或「睡眠障礙」和「執行功能*」或「抑制」或「抑制控制”或“工作記憶” ”或“靈活性”。其次,檢索相關綜述文章的參考文獻清單。當研究標題與本綜述相關時,第一作者將根據資格標準篩選摘要和全文。
Data Sources, Studies Sections, and Data Extraction
資料來源、研究部分與資料擷取
For the qualitative synthesis, data on a number of procedural variables were extracted by the first author from included studies including demographic and clinical characteristics of the sample, as well as methodological variables. Given the importance of objective sleep duration which is hypothesised to contribute to executive dysfunction (Fernandez-Mendoza et al., 2010; Vgontzas et al., 2013), information about group differences between individuals with insomnia and controls on total sleep time (TST) based on polysomnographic or actigraphic recordings were extracted, together with information about objective sleep efficiency (SE). TST is generally calculated as time spent in bed during the night (total bed time, TBT) minus the time needed to fall asleep, the wake after sleep onset and early morning awakenings. SE is then calculated as TST/TBT*100 (Carney et al., 2012). For the meta-analysis, means and standard deviations of the indices of performance reported in the included studies were extracted by the first author to compute effect sizes. When means and standard deviations were not reported in the studies, effect sizes were computed from means and standard errors. Effect sizes were not estimated from graphs. To identify and categorise the neuropsychological tests, we referred to recent systematic reviews on the topic (Diamond, 2013; Snyder et al., 2015) and consulted systematic reviews and meta-analyses on cognitive impairment in insomnia (Shekleton et al., 2010; Fortier-Brochu et al., 2012). Due to variations in test categorisation in the domain of EFs, we decided to follow the categorisation used in the meta-analysis of Fortier-Brochu et al. (2012), drawn by two independent neuropsychologists.
為了進行定性綜合,第一作者從納入的研究中提取了許多程序變數的數據,包括樣本的人口統計和臨床特徵以及方法學變數。鑑於客觀睡眠持續時間的重要性,假設客觀睡眠持續時間會導致執行功能障礙( Fernandez-Mendoza 等人,2010 ; Vgontzas 等人,2013 ),關於失眠個體和總睡眠時間(TST)對照之間的群體差異的資訊擷取是基於多導睡眠圖或活動記錄的數據,以及有關客觀睡眠效率(SE)的資訊。 TST 通常計算為夜間在床上花費的時間(總就寢時間,TBT)減去入睡所需的時間、入睡後醒來的時間以及清晨醒來的時間。然後,SE 計算為 TST/TBT*100( Carney 等人,2012 )。對於薈萃分析,第一作者提取了納入研究中報告的績效指數的平均值和標準差,以計算效應大小。當研究中未報告平均值和標準差時,效應大小會根據平均值和標準誤差計算。效應大小不是從圖表中估計的。為了對神經心理學測驗進行識別和分類,我們參考了最近關於這個主題的系統性回顧( Diamond,2013 ; Snyder 等,2015 ),並查閱了關於失眠認知障礙的系統性回顧和統合分析( Shekleton 等, 2010 ;Snyder 等, 2015 )。由於 EF 領域的測試分類存在差異,我們決定遵循Fortier-Brochu 等人的薈萃分析中使用的分類。 (2012),由兩位獨立的神經心理學家繪製。
Data Analysis 數據分析
Two independent investigators (AB, RA) assessed risk of bias using the checklist for assessing the quality of quantitative studies (Kmet et al., 2004). This tool appraises studies on different potential areas of bias, including appropriateness of the design, method of subject selection, blinding procedure, sample size, and data analysis. Disagreements between the investigators was resolved by consensus discussion.
兩位獨立研究者(AB、RA)使用評估量化研究品質的清單評估偏倚風險( Kmet 等,2004 )。該工具評估不同潛在偏差領域的研究,包括設計的適當性、受試者選擇方法、盲法程序、樣本量和數據分析。研究者之間的分歧透過共識討論得到解決。
Given the high variability of EFs measures, findings were first summarised and discussed using narrative synthesis (Popay et al., 2006). This allowed for the discussion of the differences in study findings and how clinical and methodological variables might have influenced study results, including between group differences on objective sleep.
鑑於 EF 測量的高度變異性,首先使用敘述綜合來總結和討論研究結果( Popay 等人,2006 )。這使得可以討論研究結果的差異以及臨床和方法學變數如何影響研究結果,包括客觀睡眠的組間差異。
When variability in EFs measures was limited, and there was a relevant number of studies to analyse (at least 3), meta-analysis was used in addition to the narrative synthesis to statistically estimate the presence and magnitude of EFs impairments. This was possible for the EFs assessed through reasonably comparable tasks (i.e., similar paradigms and outcomes) and for studies providing data to calculate effect sizes. To limit the impact of outcome measures' variability, analyses were run separately according to outcome type, i.e., reaction times and accuracy. When there was a relevant number of studies to analyse (at least 3), we ran sensitivity analysis to investigate the impact of objective sleep impairments on EFs.
當 EF 測量的變異性有限,且有相關數量的研究需要分析(至少 3 項)時,除了敘述綜合之外,還使用薈萃分析來統計估計 EF 損傷的存在和程度。對於透過合理可比較的任務(即類似的範式和結果)評估的 EF 以及提供數據來計算效應大小的研究來說,這是可能的。為了限制結果測量變異性的影響,根據結果類型(即反應時間和準確性)單獨進行分析。當有相關數量的研究需要分析(至少 3 項)時,我們進行敏感度分析來調查客觀睡眠障礙對 EF 的影響。
For the meta-analytic calculations, standardised mean differences (Cohen's d) were estimated at 95% confidence intervals for group differences on cognitive tasks performance. Cohen's d was derived by subtracting the mean for control groups from the mean for insomnia groups and dividing the result by the pooled standard deviation. The direction of effect size values was adjusted so that negative effects always indicate poorer performance in individuals with insomnia compared to controls. Meta-analytic calculations were computed using the statistical software “Comprehensive Meta-Analysis” version 2. A fixed effects model was used following the procedure of other authors (Fortier-Brochu et al., 2012). To test heterogeneity of effects distribution (i.e., variability in the distribution of effect sizes across studies included in a meta-analysis), Cochran's Q and Higgins's I2 were calculated. Cochran's Q is computed as a weighted sum of squared differences between single study effects and the pooled effect across studies. Significant values indicate high level of heterogeneity between effects that need to be further investigated. Higgins's I2 assesses the variability in effect estimates that is due to between-study heterogeneity rather than to chance. Low percentages of I2 are indicative of low heterogeneity while percentages over 75% represent considerable levels of heterogeneity.
對於薈萃分析計算,在認知任務表現的群體差異的 95% 置信區間內估計標準化平均差異 (Cohen's d )。 Cohen's d是從失眠組的平均值中減去對照組的平均值並將結果除以匯總標準差得出的。調整效果大小值的方向,以便負面效果總是顯示失眠個體與對照組相比表現較差。使用統計軟體「綜合薈萃分析」版本 2 進行薈萃分析計算。為了測試效應分佈的異質性(即薈萃分析中包含的各研究的效應大小分佈的變異性),計算了 Cochran's Q和 Higgins's I 2 。 Cochran's Q計算為單一研究效果與跨研究的總結效果之間的加權平方和。顯著值表示效應之間存在高度異質性,需要進一步研究。 Higgins 的I 2評估了效果估計的變異性,這是由於研究間的異質性而不是偶然造成的。 I 2的百分比低表示異質性低,而百分比超過 75% 表示異質性水準相當高。
Additionally, we performed a series of subgroup analyses including either studies that reported significant sleep differences (objective TST or SE) between those with insomnia and good sleepers or studies reporting comparable sleep values between groups in order to investigate the differences in effect sizes between these sets of studies. This allowed us to investigate the effects of insomnia with objective sleep impairment vs. insomnia with normal sleep on EFs.
此外,我們進行了一系列亞組分析,包括報告失眠者和睡眠良好者之間顯著睡眠差異(客觀TST 或SE)的研究,或報告組間可比較睡眠值的研究,以調查這些組之間效應大小的差異的研究。這使我們能夠研究客觀睡眠障礙失眠與正常睡眠失眠對 EF 的影響。
Results 結果
Study Selection and Characteristics
研究選擇和特點
The study selection flowchart is reported in Figure 1. A detailed description of study characteristics is provided in Table 1. Database search yielded 2012 studies (PubMed = 493, PsycINFO = 405, Medline = 467, Scopus n = 647). After removing duplicates, 1,625 records were identified. Reference screening yielded 16 additional records. In sum, 429 abstracts and 65 full-texts were screened against the eligibility criteria. Thirty-six studies were excluded because of the absence of: measures of inhibitory control, working memory or cognitive flexibility (n = 7), a group of individuals with standardized diagnosis of insomnia disorder (n = 15), and a control group (n = 5). A further eight studies were excluded as these allowed participants to take drugs or psychoactive substances (e.g., caffeine or alcohol) prior to assessment. Furthermore, one study was excluded due to it being a secondary analysis of a study already included for review (see Document S1 for excluded studies). Finally, 28 studies met the inclusion criteria and were included in the systematic review.
研究選擇流程圖如圖 1所示。表 1提供了研究特徵的詳細描述。資料庫檢索產生了 2012 年的研究(PubMed = 493、PsycINFO = 405、Medline = 467、Scopus n = 647)。刪除重複項後,識別出 1,625 筆記錄。參考篩選產生了 16 筆額外記錄。總之,根據資格標準篩選了 429 篇摘要和 65 篇全文。 36 項研究被排除,因為缺乏:抑制控制、工作記憶或認知靈活性的測量( n = 7)、一組具有失眠障礙標準化診斷的個體( n = 15)和對照組( n = 5)。另外八項研究被排除,因為這些研究允許參與者在評估之前服用藥物或精神活性物質(例如咖啡因或酒精)。此外,一項研究被排除,因為它是對已納入審查的一項研究的二次分析(參見文件 S1以了解被排除的研究)。最終,28篇研究符合納入標準並納入系統性回顧。
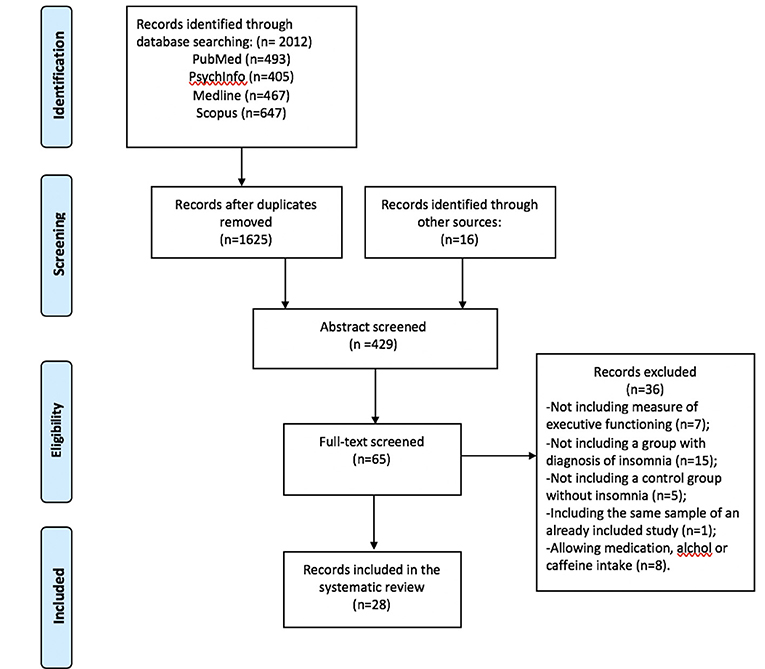
Figure 1. Flow chart for study selection.
圖1 。研究選擇的流程圖。
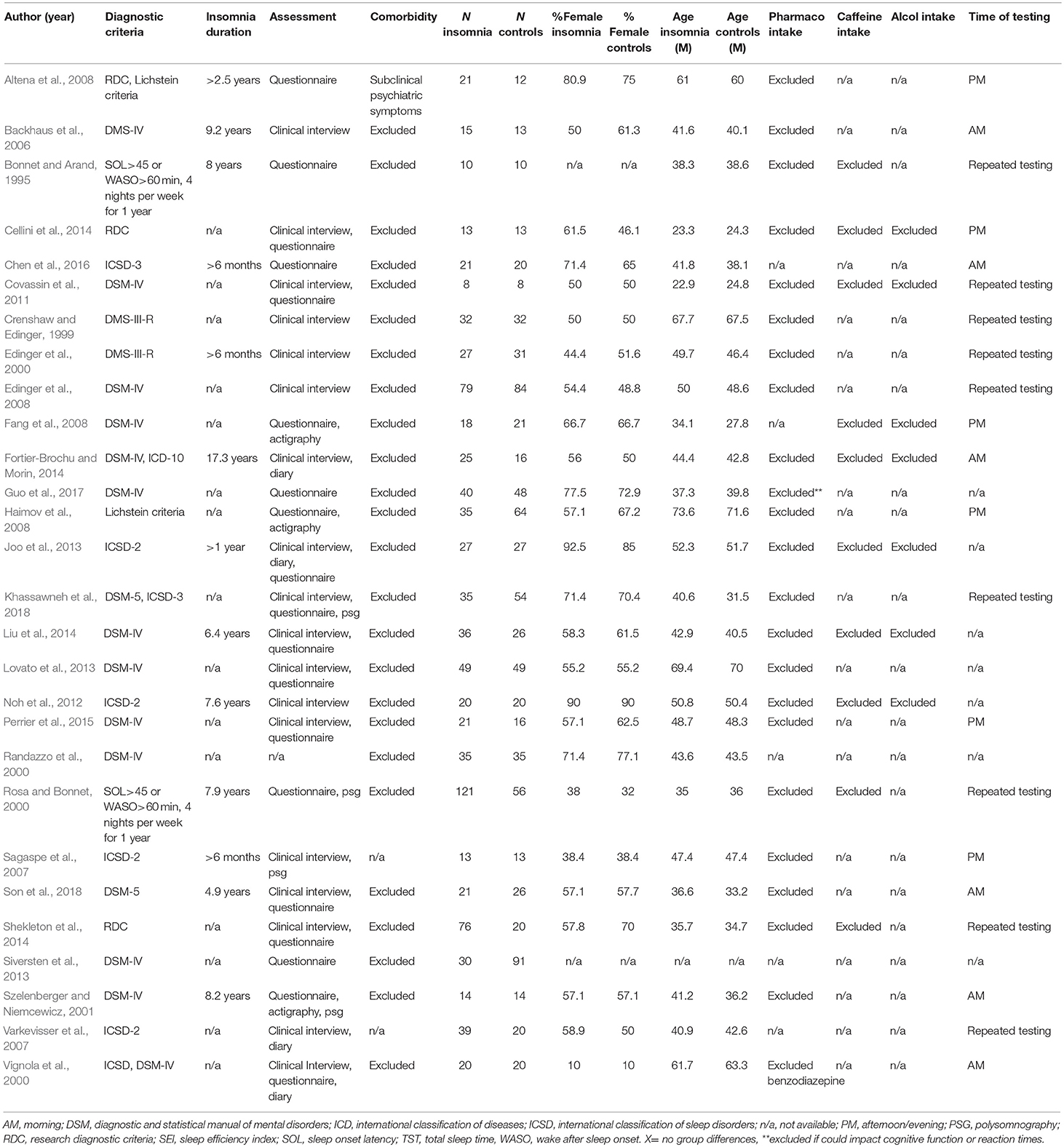
Table 1. Study characteristics.
表 1 .研究特點。
Data from 901 participants with insomnia and 859 controls were qualitatively evaluated. Mean percentage of females was 58.9 in the insomnia group and 58.5 in the controls. Mean age was 45.6 years in the insomnia group and 44.4 years in the controls.
對 901 名失眠症參與者和 859 名對照者的數據進行了定性評估。失眠組的女性平均比例為 58.9,對照組為 58.5。失眠組的平均年齡為 45.6 歲,對照組為 44.4 歲。
Synthesized Findings 綜合調查結果
Narrative Synthesis 敘事綜合
Inhibitory control 抑制控制
Thirteen studies reported a neuropsychological measure of inhibitory control as an outcome (Crenshaw and Edinger, 1999; Edinger et al., 2000, 2008; Szelenberger and Niemcewicz, 2001; Backhaus et al., 2006; Sagaspe et al., 2007; Haimov et al., 2008; Covassin et al., 2011; Joo et al., 2013; Siversten et al., 2013; Fortier-Brochu and Morin, 2014; Liu et al., 2014; Perrier et al., 2015). Three of these measured inhibitory control through the continuous performance test (Crenshaw and Edinger, 1999; Edinger et al., 2000, 2008) and one through the continuous performance test II (Fortier-Brochu and Morin, 2014). Two studies used the Stroop test (Haimov et al., 2008; Joo et al., 2013), one a similar colour-word interference test (Siversten et al., 2013) and two the stop-signal task (Sagaspe et al., 2007; Covassin et al., 2011). The attention network test, which evaluates three attention networks (alerting, orienting, executive control) was used by two studies (Liu et al., 2014; Perrier et al., 2015). Finally, one study used the go/no-go paradigm (Backhaus et al., 2006).
十三項研究報告了抑制控制的神經心理學測量結果( Crenshaw 和 Edinger,1999 ; Edinger 等,2000,2008 ; Szelenberger 和 Niemcewicz,2001 ; Backhaus 等,2006 ; Sagaspe 等,2007 ; Haimov 等等人,2008 ; Joo 等人,2013 ; Fortier-Brochu 等人,2014 ;Perrier等人,2015 。其中三個透過連續表現測試( Crenshaw 和 Edinger,1999 ; Edinger 等人,2000、2008 )測量抑制控制,一個透過連續表現測試 II( Fortier-Brochu 和 Morin,2014 )測量抑制控制。兩項研究使用了 Stroop 測試( Haimov 等人,2008 年; Joo 等人,2013 年),一項研究使用了類似的顏色詞幹擾測試( Siversten 等人,2013 年),兩項研究使用了停止信號任務( Sagaspe 等人,2013 年) 。兩項研究使用了注意力網絡測試,該測試評估了三種注意力網絡(警報、定向、執行控制)( Liu et al., 2014 ; Perrier et al., 2015 )。最後,一項研究使用了 go/no-go 範式( Backhaus et al., 2006 )。
Six of thirteen studies reported significant differences between individuals with insomnia and controls on inhibitory performance and objective sleep (see below, Haimov et al., 2008; Covassin et al., 2011; Joo et al., 2013; Fortier-Brochu and Morin, 2014; Liu et al., 2014; Perrier et al., 2015).
十三項研究中的六項報告了失眠個體與對照者在抑製表現和客觀睡眠方面存在顯著差異(見下文, Haimov 等人,2008 年; Covassin 等人,2011 年; Joo 等人,2013 年; Fortier-Brochu 和 Morin, 2014 ;劉等人,2014 ;佩里爾等人,2015 )。
Covassin et al. (2011) found that young adults with insomnia showed longer reaction times at the stop trials of the stop-signal task indicating poorer inhibitory control. However, in terms of accuracy, no differences were found. In contrast, Fortier-Brochu and Morin (2014) found that participants with insomnia differed from good sleepers in the number of perseverative errors of the continuous performance task II, but not on mean reaction times. Haimov et al. (2008) reported that individuals with insomnia showed longer reaction times in the Stroop test, consistent with Joo et al. (2013). Liu et al. (2014) found that adults with insomnia showed impaired functioning in the executive control performance of the attentional network test. In contrast, Perrier et al. (2015) found intact performance on the same task, but increased reaction times (RTs) in the incongruent Flankers compared to congruent and neutral Flankers, that they interpreted as a conflict resolution deficit. With respect to objective sleep, four of these studies reported significant shorter TST (Covassin et al., 2011; Joo et al., 2013; Fortier-Brochu and Morin, 2014; Liu et al., 2014) and two lower SE in insomnia as compared to controls (Haimov et al., 2008; Perrier et al., 2015).
科瓦辛等人。 (2011)發現,失眠的年輕人在停止訊號任務的停止試驗中表現出更長的反應時間,顯示抑制控制較差。然而,就準確性而言,沒有發現差異。相較之下, Fortier-Brochu 和 Morin (2014)發現,失眠參與者與睡眠良好的參與者在連續執行任務 II 的持續錯誤數量上存在差異,但在平均反應時間上沒有差異。海莫夫等人。 (2008)報告稱,失眠個體在 Stroop 測試中表現出更長的反應時間,這與Joo 等人的觀點一致。 (2013) 。劉等人。 (2014)發現,失眠的成年人在註意力網路測試的執行控製表現中表現出功能受損。相比之下, Perrier 等人。 (2015)發現在相同任務上表現完好,但與一致和中立的側翼相比,不一致的側翼的反應時間(RT)增加,他們將其解釋為衝突解決赤字。關於客觀睡眠,其中四項研究報告稱,失眠患者的 TST 顯著縮短( Covassin 等人,2011 ; Joo 等人,2013 ; Fortier-Brochu 和 Morin,2014 ; Liu 等人,2014 ),兩項研究的SE 較低與對照組相比( Haimov 等人,2008 ; Perrier 等人,2015 )。
Three of the eight studies that found no significant differences between individuals with insomnia and controls on inhibitory control tasks found no differences between groups on TST (Crenshaw and Edinger, 1999; Edinger et al., 2000, 2008), one in both TST and SE (Crenshaw and Edinger, 1999); three did not report information on objective sleep data (Szelenberger and Niemcewicz, 2001; Sagaspe et al., 2007; Siversten et al., 2013). Only in the study of Backhaus et al. (2006), participants with insomnia objectively slept less and worse than controls, although no effects on inhibitory control were found. Findings on inhibitory control are summarised in Table 2.
在八項研究中,三項發現失眠個體和對照組在抑制性控制任務上沒有顯著差異,發現各組之間在 TST 上沒有差異( Crenshaw 和 Edinger,1999 ; Edinger 等,2000,2008 ) ,其中一項在TST 和SE 上都沒有差異(克倫肖和艾丁格,1999 );其中三人沒有報告客觀睡眠數據的資訊( Szelenberger 和 Niemcewicz,2001 ; Sagaspe 等人,2007 ; Siversten 等人,2013 )。僅在Backhaus 等人的研究中。 (2006) ,失眠的參與者客觀上比對照組睡眠更少且更差,儘管沒有發現對抑制控制的影響。表 2總結了抑制控制的結果。
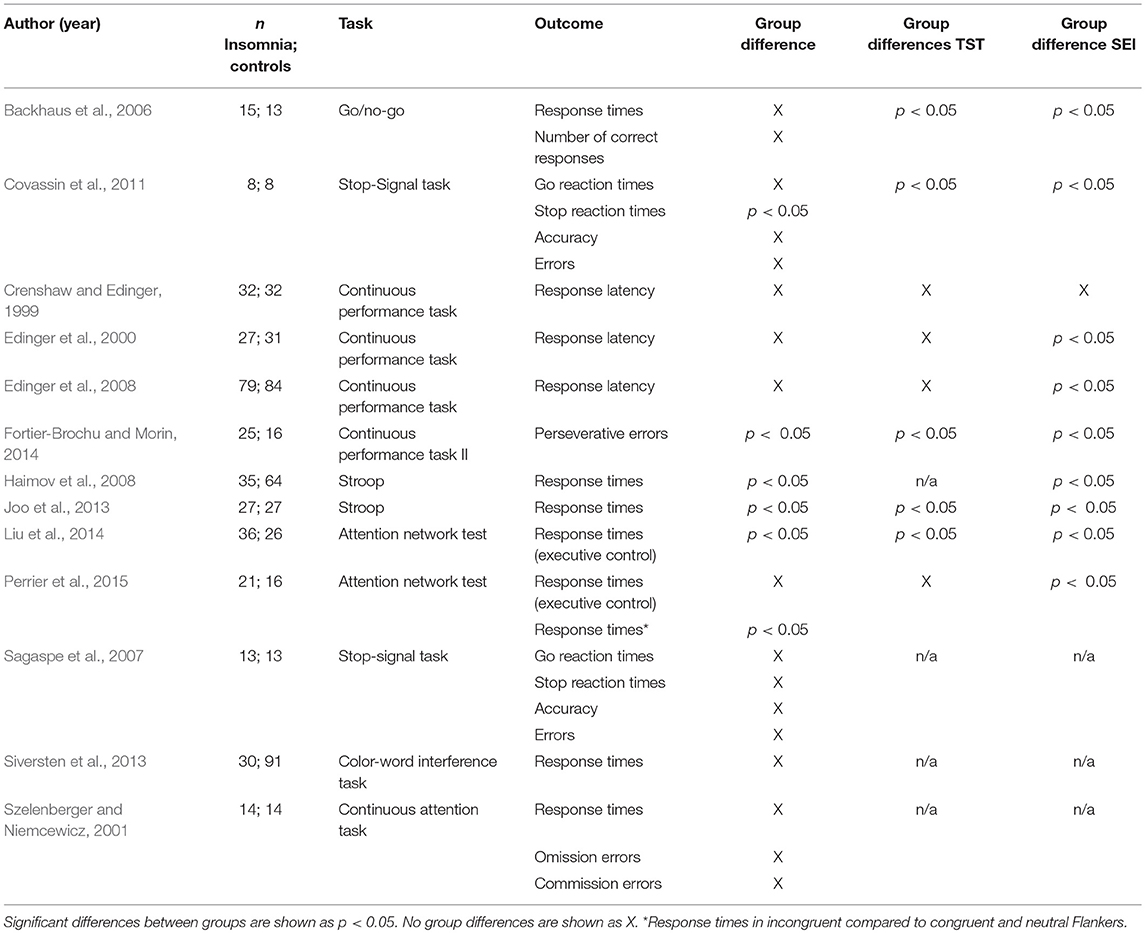
Table 2. Comparison of individuals with insomnia and controls on tasks of inhibitory control.
表 2 .失眠個體與對照組在抑制控制任務的比較。
Working Memory 工作記憶
Seventeen studies assessed working memory (Bonnet and Arand, 1995; Randazzo et al., 2000; Rosa and Bonnet, 2000; Vignola et al., 2000; Varkevisser et al., 2007; Haimov et al., 2008; Noh et al., 2012; Joo et al., 2013; Lovato et al., 2013; Siversten et al., 2013; Cellini et al., 2014; Fortier-Brochu and Morin, 2014; Shekleton et al., 2014; Chen et al., 2016; Guo et al., 2017; Khassawneh et al., 2018; Son et al., 2018). Eight of these measured working memory through digit or spatial span backward tests (Randazzo et al., 2000; Vignola et al., 2000; Haimov et al., 2008; Noh et al., 2012; Joo et al., 2013; Lovato et al., 2013; Fortier-Brochu and Morin, 2014; Khassawneh et al., 2018). Four studies used the n-back memory task (Varkevisser et al., 2007; Cellini et al., 2014; Shekleton et al., 2014; Son et al., 2018); two used the memory and search task (Bonnet and Arand, 1995; Rosa and Bonnet, 2000) two used the letter-number sequencing test (Randazzo et al., 2000; Siversten et al., 2013), one used the Corsi block test backward (Noh et al., 2012), one used the nine box maze test to measure spatial and object working memory (Chen et al., 2016) and one the Montreal cognitive assessment battery (Guo et al., 2017).
十七項研究評估了工作記憶( Bonnet 和 Arand,1995 ; Randazzo 等,2000 ; Rosa 和 Bonnet,2000 ; Vignola 等,2000 ; Varkevisser 等,2007 ; Haimov 等,2008 ; Noh 等。 ,2012 ; Lovato 等人; ,2013 ; Siversten 等人, 2014 ; Fortier-Brochu 和 Morin 等人,2014 ; ,2016 ; Guo 等,2017 ; Khassawneh 等,2018 ; Son 等,2018 )。其中八項透過數字或空間跨度向後測試來測量工作記憶( Randazzo 等人,2000 ; Vignola 等人,2000 ; Haimov 等人,2008 ; Noh 等人,2012 ; Joo 等人,2013 ; Lovato等人, 2013 ; Fortier-Brochu 和 Morin,2014 ; Khassawneh 等人,2018 )。四項研究使用了 n-back 記憶任務( Varkevisser 等人,2007 年; Cellini 等人,2014 年; Shekleton 等人,2014 年; Son 等人,2018 年);兩個使用記憶和搜尋任務( Bonnet 和 Arand,1995 ; Rosa 和 Bonnet,2000 ),兩個使用字母數字排序測試( Randazzo 等,2000 ; Siversten 等,2013 ),一個使用 Corsi 區塊測試向後( Noh等人,2012 ),一種使用九盒迷宮測試來測量空間和物體工作記憶( Chen等人,2016 ),一種使用蒙特利爾認知評估電池( Guo等人,2017 )。
Nine out of seventeen studies showed significant differences between individuals with insomnia and good sleeper controls on performance (Bonnet and Arand, 1995; Randazzo et al., 2000; Vignola et al., 2000; Haimov et al., 2008; Noh et al., 2012; Joo et al., 2013; Lovato et al., 2013; Cellini et al., 2014; Chen et al., 2016). Of these nine, sleep was objectively impaired in four (Bonnet and Arand, 1995; Haimov et al., 2008; Joo et al., 2013; Cellini et al., 2014). Seven out of seventeen studies did not report information on objective sleep (Randazzo et al., 2000; Varkevisser et al., 2007; Lovato et al., 2013; Siversten et al., 2013; Shekleton et al., 2014; Chen et al., 2016; Guo et al., 2017). With respect to the tasks, performance was consistently impaired in digit and spatial span backward tests, with the exception of two studies (Randazzo et al., 2000; Fortier-Brochu and Morin, 2014). However, Randazzo et al. (2000) found significant impairments in insomnia vs. controls on spatial, but not digit span tasks. The two studies using the two-back memory task failed to find significant differences between individuals with insomnia and controls (Varkevisser et al., 2007; Son et al., 2018). The majority of the studies (five out of eight) which did not report significant differences between subjects with insomnia and controls did not report data on objective sleep (Randazzo et al., 2000; Varkevisser et al., 2007; Siversten et al., 2013; Shekleton et al., 2014; Guo et al., 2017). Findings on working memory are summarised in Table 3.
十七項研究中的九項表明,失眠者和睡眠控制良好的個體在表現方面存在顯著差異( Bonnet 和 Arand,1995 ; Randazzo 等,2000 ; Vignola 等,2000 ; Haimov 等,2008 ; Noh 等, 2000 ) 。在這九人中,有四人的睡眠客觀上受到損害( Bonnet 和 Arand,1995 ; Haimov 等,2008 ; Joo 等,2013 ; Cellini 等,2014 )。十七項研究中有七項沒有報告客觀睡眠的資訊( Randazzo 等人,2000 年; Varkevisser 等人,2007 年; Lovato 等人,2013 年; Siversten 等人,2013 年; Shekleton 等人,2014 年; Chen 等)等,2016 ;郭等,2017 )。就任務而言,除了兩項研究之外,數字和空間跨度向後測試中的表現始終受到損害( Randazzo 等人,2000 年; Fortier-Brochu 和 Morin,2014 年)。然而,蘭達佐等。 (2000)發現失眠與空間控制相比有顯著損害,但數字跨度任務沒有顯著損害。使用雙背記憶任務的兩項研究未能發現失眠個體和對照組之間的顯著差異( Varkevisser 等,2007 ; Son 等,2018 )。大多數研究(八分之五)沒有報告失眠受試者和對照組之間的顯著差異,也沒有報告客觀睡眠數據( Randazzo 等人,2000 年; Varkevisser 等人,2007 年; Siversten 等人, 2007 年)。, 2013 ;謝克爾頓等人,2014 ;郭等人,2017 )。表 3總結了工作記憶的研究結果。
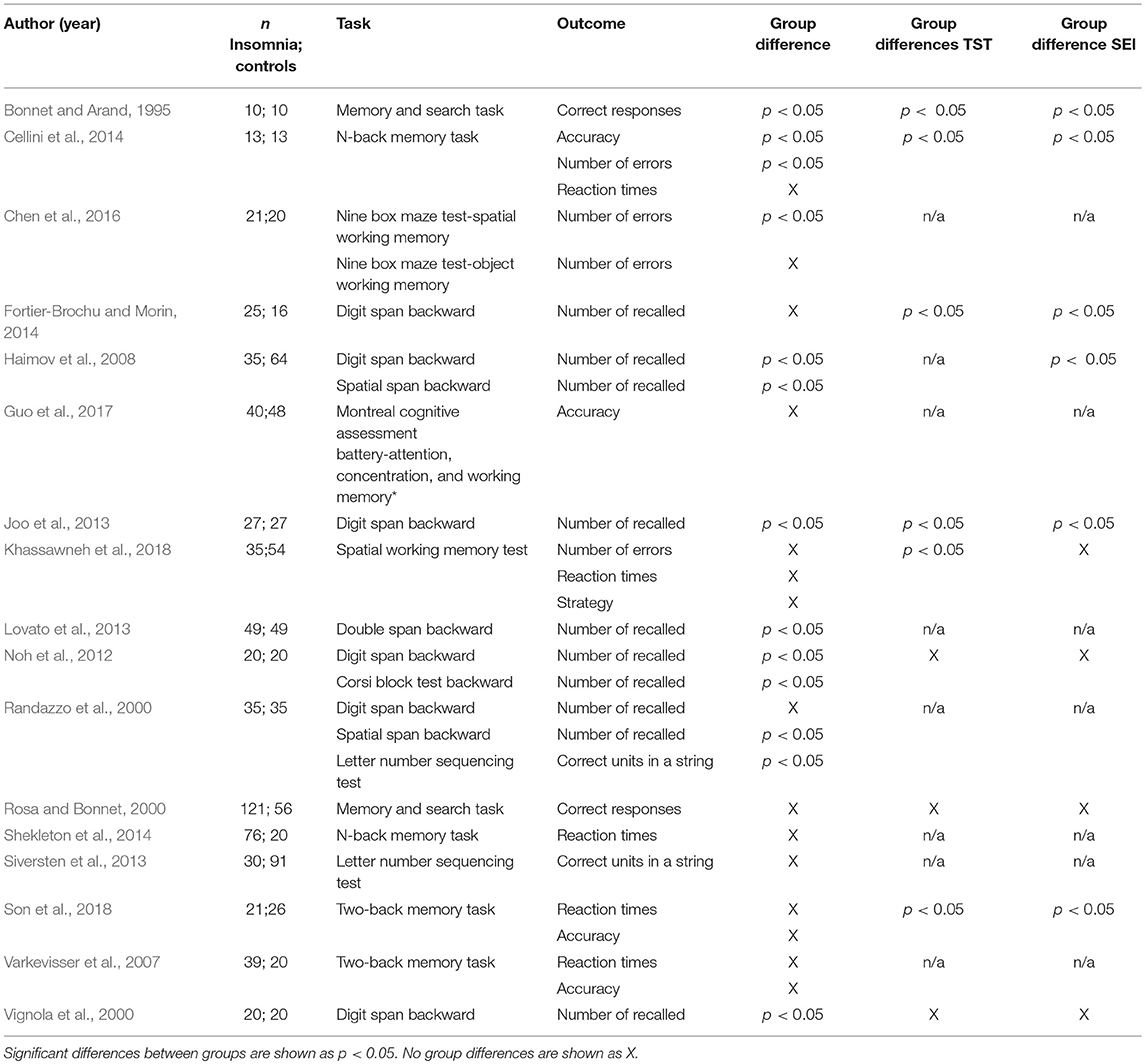
Table 3. Comparison of individuals with insomnia and controls on tasks of working memory.
表 3 .失眠個體與工作記憶任務控制的比較。
Cognitive Flexibility 認知彈性
Twelve studies reported a measure of cognitive flexibility (Edinger et al., 2000, 2008; Vignola et al., 2000; Altena et al., 2008; Fang et al., 2008; Noh et al., 2012; Joo et al., 2013; Siversten et al., 2013; Fortier-Brochu and Morin, 2014; Shekleton et al., 2014; Guo et al., 2017; Khassawneh et al., 2018). Four studies measured flexibility through switching attention tasks (Edinger et al., 2000, 2008; Shekleton et al., 2014; Khassawneh et al., 2018) and using verbal fluency tasks (Vignola et al., 2000; Siversten et al., 2013; Fortier-Brochu and Morin, 2014). The Wisconsin card sorting test was used in two studies (Vignola et al., 2000; Fang et al., 2008), as well as the controlled oral word association test (Noh et al., 2012; Joo et al., 2013). The trail making test B was used in two studies (Joo et al., 2013; Siversten et al., 2013). Finally, one study used the “visuospatial and executive function” subtest of the Montreal cognitive assessment battery, based on the trail making test B, verbal fluency task and verbal abstraction task (Guo et al., 2017).
十二項研究報告了認知彈性的衡量標準( Edinger 等人,2000 年、 2008 年; Vignola 等人,2000 年; Altena 等人,2008 年; Fang 等人,2008 年; Noh 等人,2012年; Joo 等人, 2012年) 。四項研究透過切換注意力任務( Edinger 等人,2000 年、 2008 年; Shekleton 等人,2014 年; Khassawneh 等人,2018 年)和使用語言流暢性任務( Vignola 等人,2000 年; Siversten 等人, 2013 ;福蒂爾-布羅楚和莫林,2014 )。兩項研究中使用了威斯康辛卡片分類測驗( Vignola et al., 2000 ; Fang et al., 2008 ),以及受控口語單字關聯測驗( Noh et al., 2012 ; Joo et al., 2013 ) 。兩項研究中使用了路線測試 B( Joo 等人,2013 年; Siversten 等人,2013 年)。最後,一項研究使用了蒙特利爾認知評估組的「視覺空間和執行功能」子測試,基於軌跡製作測試B、言語流暢性任務和言語抽象任務( Guo et al., 2017 )。
Four of twelve studies reported significant differences between individuals with insomnia and good sleepers in some aspects of performance (Edinger et al., 2000, 2008; Noh et al., 2012; Khassawneh et al., 2018). Of these, three also reported between group differences on objective sleep. Specifically, Edinger et al. (2000, 2008) found significant shorter TST and Khassawneh et al. (2018) lower SE in insomnia as compared to controls. Sleep was comparable between the groups in the study of Noh et al. (2012).
十二項研究中有四項報告稱,失眠者和睡眠良好者在某些方面的表現存在顯著差異( Edinger 等人,2000 年、 2008 年; Noh 等人,2012 年; Khassawneh 等人,2018年)。其中,三人也報告了客觀睡眠的組間差異。具體來說, Edinger 等人。 (2000 , 2008)發現 TST 顯著縮短, Khassawneh 等人。 (2018)與對照組相比,失眠患者的 SE 較低。 Noh 等人的研究中,各組之間的睡眠情況相當。 (2012) 。
Edinger et al. (2000) found that individuals with insomnia showed longer response latency in the switching attention test part III, and the result was replicated by a later study by the same group (Edinger et al., 2008). Similarly, Khassawneh et al. (2018) found slower response latency and higher number of incorrect trials in a similar task. However, Shekleton et al. (2014) replicated the result only in individuals with insomnia and short sleep duration, and no changes to performance was found in subjects with insomnia and normal sleep duration. Fortier-Brochu and Morin (2014) failed to find between group differences in a verbal fluency test. Instead, Noh et al. (2012) found that individuals with insomnia produced less words than controls in the controlled oral association test, reflecting poorer flexibility. However, other researchers failed to replicate these results using similar tests (Altena et al., 2008; Siversten et al., 2013). Performance on the trail making test B (Noh et al., 2012; Joo et al., 2013) and the Wisconsin card sorting test (Vignola et al., 2000; Fang et al., 2008) of individuals with insomnia remained comparable to the controls.
埃丁格等。 (2000)發現失眠個體在註意力轉換測試第三部分中表現出更長的反應潛伏期,並且該結果被同一小組後來的研究複製( Edinger et al., 2008 )。同樣,哈蘇奈等人。 (2018)發現在類似任務中反應延遲較慢且錯誤試驗次數較多。然而,謝克萊頓等人。 (2014)僅在失眠和睡眠時間短的個體中複製了結果,並且在失眠和睡眠時間正常的受試者中沒有發現表現發生變化。 Fortier-Brochu 和 Morin(2014)未能在言語流暢性測驗中發現群體之間的差異。相反, Noh 等人。 (2012)發現,在受控口語聯想測驗中,失眠者比對照組產生的單字更少,反映出彈性較差。然而,其他研究人員未能使用類似的測試複製這些結果( Altena 等人,2008 年; Siversten 等人,2013 年)。失眠個體在追蹤測試 B( Noh 等人,2012 年; Joo 等人,2013 年)和威斯康辛州卡片分類測試( Vignola 等人,2000 年; Fang 等人,2008 年)上的表現仍然與控制。
Only three of the eight studies which failed to find significant differences between individuals with insomnia and controls on EFs reported significant differences in TST and SE (Fang et al., 2008; Joo et al., 2013; Fortier-Brochu and Morin, 2014). Vignola et al. (2000) reported no differences on objective TST and SE between those with insomnia and controls, while Altena et al. (2008), Siversten et al. (2013) and Guo et al. (2017) did not provide data on objective sleep measurement. Findings on cognitive flexibility are summarised in Table 4.
在未能發現失眠個體與 EF 對照組之間顯著差異的八項研究中,只有 3 項報告了 TST 和 SE 的顯著差異( Fang 等人,2008 ; Joo 等人,2013 ; Fortier-Brochu 和Morin ,2014 ) 。維尼奧拉等人。 (2000)報告稱,失眠患者和對照組之間的客觀 TST 和 SE 沒有差異,而Altena 等人。 (2008) , Siversten 等人。 (2013)和郭等人。 (2017)沒有提供客觀睡眠測量的數據。表 4總結了關於認知靈活性的調查結果。
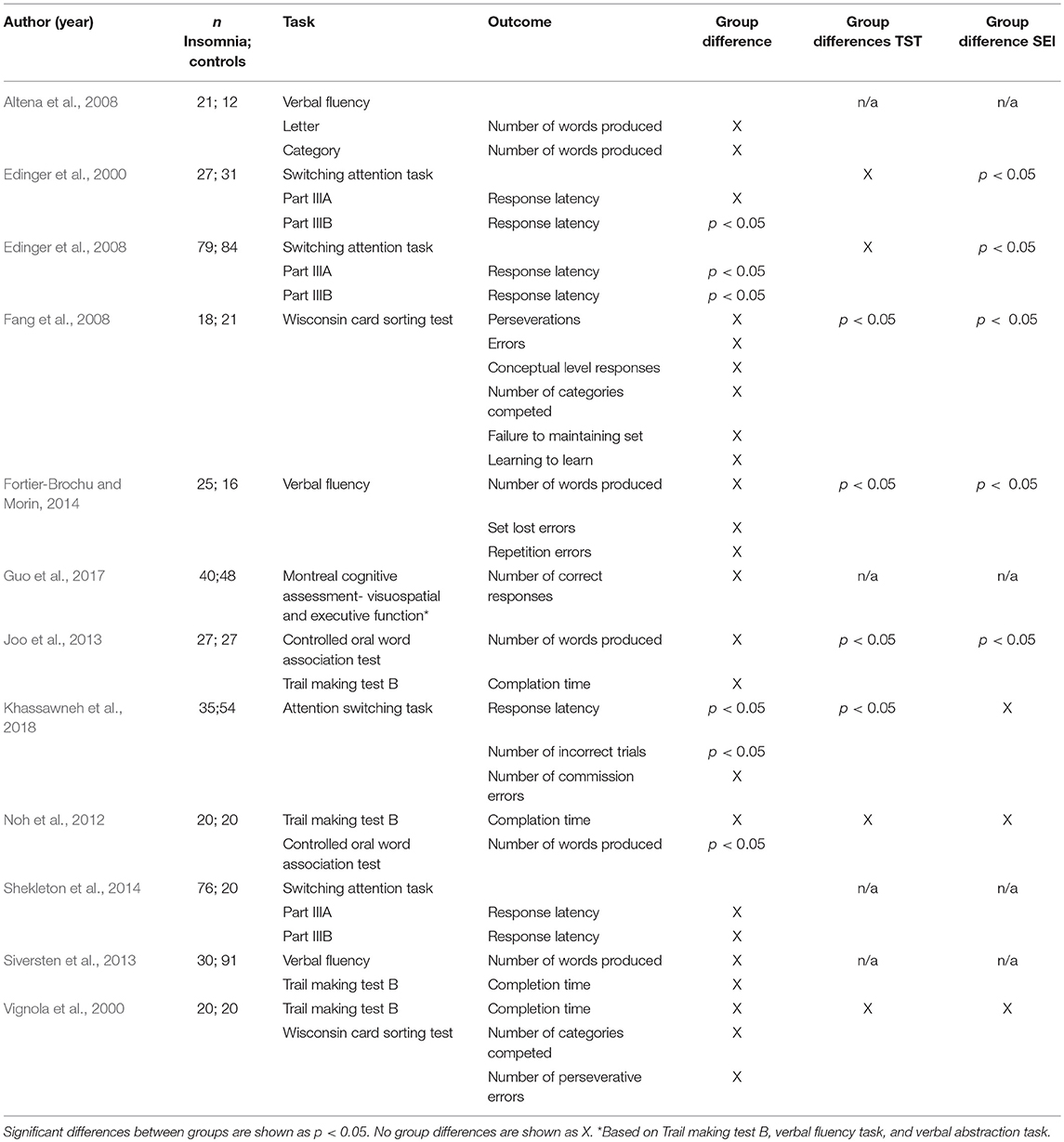
Table 4. Comparison of individuals with insomnia and controls on tasks of cognitive flexibility.
表 4 .失眠個體與對照個體在認知彈性任務上的比較。
Exploratory Meta-Analysis
探索性薈萃分析
Inhibitory Control 抑制控制
Nine of thirteen studies measuring inhibitory control provided data to compute effect sizes (Crenshaw and Edinger, 1999; Edinger et al., 2000; Szelenberger and Niemcewicz, 2001; Backhaus et al., 2006; Sagaspe et al., 2007; Covassin et al., 2011; Siversten et al., 2013; Liu et al., 2014; Perrier et al., 2015). These reported reaction times as an outcome. Additionally, four of nine studies included a measure of accuracy of the performance (Szelenberger and Niemcewicz, 2001; Backhaus et al., 2006; Sagaspe et al., 2007; Covassin et al., 2011). Thus, we conducted separate analyses for reaction times and accuracy. Reaction times were significantly slower for individuals with insomnia (n = 303) than controls (n = 355) (d = −0.32, 95% CI: −0.52 to −0.13). Heterogeneity statistics were non-significant, showing that the distribution of effects across studies was homogeneous (Q = 3.328, df = 8, p = 0.912; I2 = 0.000%). Forest plot of analysis is reported in Figure 2.
測量抑制控制的 13 項研究中有 9 項提供了計算效應大小的數據( Crenshaw 和 Edinger,1999 ; Edinger 等,2000 ; Szelenberger 和 Niemcewicz,2001 ; Backhaus 等,2006 ; Sagaspe 等,2007 ; Covassin 等) . , 2011 ; Siversten 等人, 2013 ; Liu 等人, 2014 ; Perrier 等人, 2015 )。這些報告的反應時間作為結果。此外,九項研究中有四項包括對錶現準確性的測量( Szelenberger 和 Niemcewicz,2001 ; Backhaus 等人,2006 ; Sagaspe 等人,2007 ; Covassin 等人,2011 )。因此,我們對反應時間和準確性進行了單獨分析。失眠患者 ( n = 303) 的反應時間明顯慢於對照組 ( n = 355)( d = -0.32,95% CI:-0.52 至 -0.13)。異質性統計不顯著,顯示研究之間的效應分佈是同質的( Q = 3.328,df = 8, p = 0.912; I 2 = 0.000%)。分析森林圖如圖 2所示。
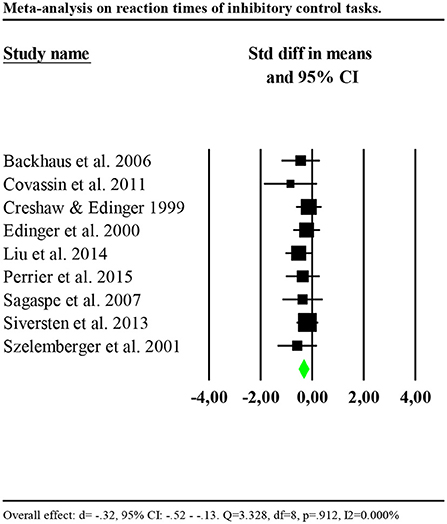
Figure 2. Forest plot of the meta-analysis on reaction times of inhibitory control. Results are presented as standardised mean differences (Std diff) and 95% confidence intervals (CI).
圖2 .抑制控制反應時間薈萃分析的森林圖。結果以標準化平均差 (Std diff) 和 95% 信賴區間 (CI) 形式呈現。
We investigated whether the effect size was larger for studies including participants with insomnia and objective sleep impairment (shorter TST or lower SE compared to the controls) by including only these studies in the analysis (Edinger et al., 2000; Backhaus et al., 2006; Covassin et al., 2011; Liu et al., 2014; Perrier et al., 2015). Results showed a significant and larger effect (d = −0.41, 95% CI: −0.69 to −0.13). Heterogeneity statistics were non-significant (Q = 1.436, df = 4, p = 0.838; I2 = 0.000%). In contrast, including only studies which failed to find significant differences between insomnia and control groups or missed to report information on objective sleep (Crenshaw and Edinger, 1999; Szelenberger and Niemcewicz, 2001; Sagaspe et al., 2007; Siversten et al., 2013), results showed a smaller effect (d = −0.24, 95% CI: −0.51 to −0.03), with low and non-significant heterogeneity (Q = 1.144, df = 3, p = 0.766; I2 = 0.000%).
我們透過僅將這些研究納入分析來調查包括失眠和客觀睡眠障礙參與者(與對照組相比較短的 TST 或較低的 SE)的研究的效應大小是否更大( Edinger 等人,2000 年; Backhaus等人, 2006 ; Covassin 等人,2011 ; Liu 等人,2014 ; Perrier 等人,2015 )。結果顯示效果顯著且更大( d = -0.41,95% CI:-0.69 至 -0.13)。異質性統計不顯著( Q = 1.436,df = 4, p = 0.838; I 2 = 0.000%)。相較之下,僅包括未能發現失眠和對照組之間存在顯著差異或錯過報告客觀睡眠資訊的研究( Crenshaw 和 Edinger,1999 ; Szelenberger 和 Niemcewicz,2001 ; Sagaspe 等,2007 ; Siversten 等,2013 ),結果顯示影響較小( d = -0.24,95% CI:-0.51 至 -0.03),異質性較低且不顯著( Q = 1.144,df = 3, p = 0.766; I 2 = 0.000 % )。
Results on accuracy showed that the performance of individuals with insomnia was significantly more accurate than that of controls (d = 0.504, 95% CI: 0.082 to 0.925). Nevertheless, effects distribution was significantly heterogenous between studies (Q = 19.162, df = 3, p<0.001; I2 = 84.344%). We repeated the analysis removing one potential outlier (Covassin et al., 2011, d = 0.4.21, 95% CI: 2.38–5.85). Results showed smaller and no longer significant effect (d = 0.27, 95% CI: −0.15 to 0.71). Heterogeneity tests were low and no longer significant, reflecting a homogeneous distribution of the effects across studies (Q = 1.345, df = 2, p = 0.510; I2 = 0.000%). Forest plot of the analysis is reported in Figure 3. Given the small number of studies, we were limited in performing further sensitivity analyses.
準確度結果表明,失眠個體的表現明顯比對照組更準確( d = 0.504,95% CI:0.082 至 0.925)。然而,研究之間的效應分佈存在顯著異質性( Q = 19.162,df = 3, p < 0.0 01; I 2 = 84.344%)。我們重複了分析,刪除了一個潛在的異常值( Covassin 等人,2011 , d = 0.4.21,95% CI:2.38–5.85)。結果顯示影響較小且不再顯著( d = 0.27,95% CI:-0.15 至 0.71)。異質性檢定較低且不再顯著,反映出研究中效果的均勻分佈( Q = 1.345,df = 2, p = 0.510; I 2 = 0.000%)。分析的森林圖如圖 3所示。由於研究數量較少,我們在進行進一步的敏感度分析方面受到限制。
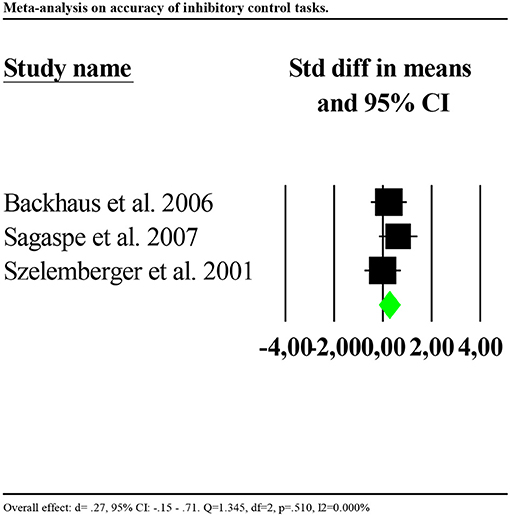
Figure 3. Forest plot of the meta-analysis on accuracy of inhibitory control (outlier removed). Results are presented as standardised mean differences (Std diff) and 95% confidence intervals (CI).
圖3 .抑制控制準確性薈萃分析的森林圖(已刪除異常值)。結果以標準化平均差 (Std diff) 和 95% 信賴區間 (CI) 形式呈現。
Working Memory 工作記憶
Eight studies reported data of accuracy of the performance (Bonnet and Arand, 1995; Rosa and Bonnet, 2000; Lovato et al., 2013; Cellini et al., 2014; Fortier-Brochu and Morin, 2014; Guo et al., 2017; Khassawneh et al., 2018; Son et al., 2018). Only one study reported data for reaction times (Cellini et al., 2014). Consequently, we performed the analysis for accuracy only. Analysis showed no significant results (d = −0.034, 95% CI: −0.211 to 0.144) and high heterogeneity (Q = 42.678, df = 6, p < 0.001; I2 = 85.941%). We repeated the analysis removing one potential outlier (Khassawneh et al., 2018, d = −1.161, 95% CI: −1.93 to −0.98). Results showed a small significant effect (d = −0.19, 95% CI: −0.38 to −0.00). Heterogeneity statistics were not significant (Q = 2.645, df = 5, p = 0.754; I2 = 0.000%). Forest plot of this analysis is reported in Figure 4.
八項研究報告了性能準確性的數據( Bonnet 和 Arand,1995 ; Rosa 和 Bonnet,2000 ; Lovato 等,2013 ; Cellini 等,2014 ; Fortier-Brochu 和 Morin,2014 ; Guo 等,2017) ; Khassawneh 等人,2018 ; Son 等人,2018 )。只有一項研究報告了反應時間數據( Cellini 等,2014 )。因此,我們僅出於準確性進行分析。分析顯示沒有顯著結果( d = -0.034,95% CI:-0.211 至 0.144)和高異質性( Q = 42.678,df = 6, p < 0.001; I 2 = 85.941%)。我們重複了分析,刪除了一個潛在的異常值( Khassawneh 等人,2018 , d = -1.161,95% CI:-1.93 至 -0.98)。結果顯示有較小的顯著影響( d = -0.19,95% CI:-0.38 至 -0.00)。異質性統計不顯著( Q = 2.645,df = 5, p = 0.754; I 2 = 0.000%)。此分析的森林圖如圖 4所示。
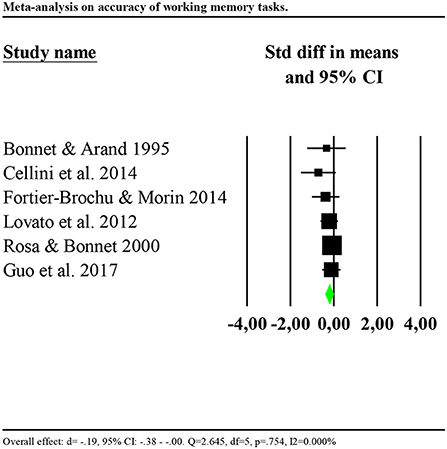
Figure 4. Forest plot of the meta-analysis on accuracy of working memory (outlier removed). Results are presented as standardised mean differences (Std diff) and 95% confidence intervals (CI).
圖4 .工作記憶準確性薈萃分析的森林圖(已刪除異常值)。結果以標準化平均差 (Std diff) 和 95% 信賴區間 (CI) 形式呈現。
We investigated whether the effect was larger for studies including participants with insomnia and objective sleep impairment (shorter TST or lower SE compared to the controls) by including only these in the analysis (Bonnet and Arand, 1995; Cellini et al., 2014; Fortier-Brochu and Morin, 2014). Results showed a significant and larger effect (d = −0.46, 95% CI: −0.03 to −0.89). Heterogeneity statistics were non-significant (Q = 0.525, df = 2, p = 0.769; I2 = 0.000%). In contrast, including only studies which failed to find significant differences between insomnia and control groups, or missed to report information on objective sleep, showed a smaller and non-significant effect (d = −0.13, 95% CI: −0.08 to 0.34), with low and non-significant heterogeneity (Q = 0.240, df = 2, p = 0.887; I2 = 0.000%).
我們透過僅將這些納入分析,調查了對於包括患有失眠和客觀睡眠障礙的參與者(與對照組相比較短的 TST 或較低的 SE)的研究,效果是否更大( Bonnet 和 Arand,1995 ; Cellini 等,2014 ; Fortier ) -Brochu 和 Morin,2014 )。結果顯示效果顯著且更大( d = -0.46,95% CI:-0.03 至 -0.89)。異質性統計不顯著( Q = 0.525,df = 2, p = 0.769; I 2 = 0.000%)。相較之下,僅包括未能發現失眠和對照組之間存在顯著差異或錯過報告客觀睡眠資訊的研究,顯示出較小且不顯著的影響( d = -0.13,95% CI:- 0.08至0.34) ,具有低且不顯著的異質性( Q = 0.240,df = 2, p = 0.887; I 2 = 0.000%)。
Cognitive Flexibility 認知彈性
Four studies reported reaction times (Edinger et al., 2000; Vignola et al., 2000; Siversten et al., 2013; Khassawneh et al., 2018) and four accuracy (Fang et al., 2008; Fortier-Brochu and Morin, 2014; Guo et al., 2017; Khassawneh et al., 2018) as outcomes. Consequently, we ran separate analyses for reaction times and accuracy. Reaction times were significantly slower for individuals with insomnia as compared to controls (d = −0.77, 95% CI: −1.03 to −0.51). Nevertheless, the distribution of effects was highly and significantly heterogenous between studies (Q = 54.954, df = 3, p < 0.001; I2 = 94.541). We repeated the analysis removing one potential outlier (Khassawneh et al., 2018, d = −2.689, 95% CI: −3.26 to −2.10). Results showed a significant effect (d = −0.30, 95% CI: −0.59 to −0.01). Heterogeneity tests were low and no longer significant (Q = 2.920, df = 2, p = 0.232; I2 = 31.496). Forest plot of this analysis is reported in Figure 5.
四項研究報告了反應時間( Edinger 等人,2000 年; Vignola 等人,2000 年; Siversten 等人,2013 年; Khassawneh 等人,2018 年)和四個準確度( Fang 等人,2008 年; Fortier -Brochu 和Morin) ,2014 ; Guo 等人,2017 ; Khassawneh 等人,2018 )作為結果。因此,我們對反應時間和準確性進行了單獨的分析。與對照組相比,失眠個體的反應時間明顯較慢( d = -0.77,95% CI:-1.03 至 -0.51)。然而,研究之間的效應分佈存在高度且顯著的異質性( Q = 54.954,df = 3, p < 0.001; I 2 = 94.541)。我們重複了分析,刪除了一個潛在的異常值( Khassawneh et al., 2018 , d = -2.689,95% CI:-3.26 至 -2.10)。結果顯示有顯著效果( d = -0.30,95% CI:-0.59 至 -0.01)。異質性檢定較低且不再顯著( Q = 2.920,df = 2, p = 0.232; I 2 = 31.496)。此分析的森林圖如圖 5所示。
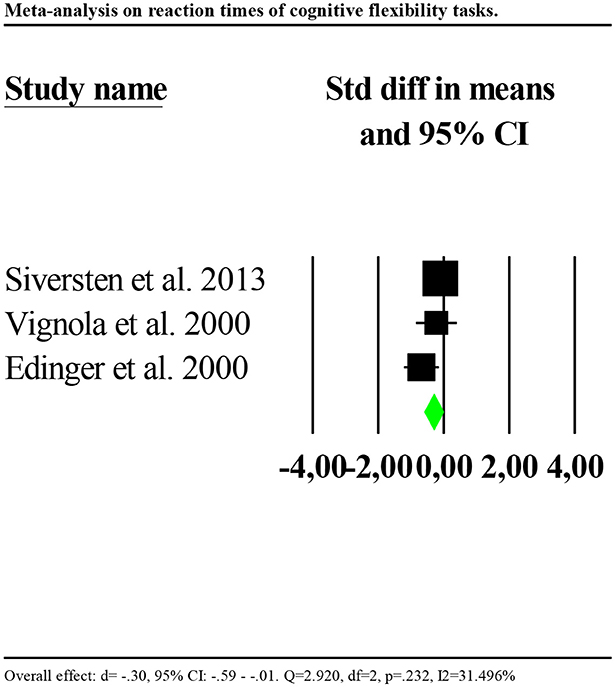
Figure 5. Forest plot of the meta-analysis on reaction times of cognitive flexibility (outlier removed). Results are presented as standardised mean differences (Std diff) and 95% confidence intervals (CI).
圖5 .認知靈活性反應時間薈萃分析的森林圖(已刪除異常值)。結果以標準化平均差 (Std diff) 和 95% 信賴區間 (CI) 形式呈現。
Accuracy was significantly poorer for individuals with insomnia than controls (d = −0.602, 95% CI: −0.873 to −0.330). Again, the distribution of effects was highly and significantly heterogenous between studies (Q = 67.580, df = 3, p < 0.001; I2 = 95.561). We repeated the analysis removing one potential outlier (Khassawneh et al., 2018, d = −2.733, 95% CI: −3.31 to −2.14). Results showed no significant effects (d = −0.017, 95% CI: −0.32 to 0.28). Heterogeneity tests were low and no longer significant (Q = 2.576, df = 2, p = 0.276; I2 = 22.375). Forest plot of this analysis is reported in Figure 6.
失眠個體的準確度明顯低於對照組( d = -0.602,95% CI:-0.873 至 -0.330)。同樣,研究之間的效應分佈具有高度且顯著的異質性( Q = 67.580,df = 3, p < 0.001; I 2 = 95.561)。我們重複了分析,刪除了一個潛在的異常值( Khassawneh 等人,2018 , d = -2.733,95% CI:-3.31 至 -2.14)。結果顯示沒有顯著影響( d = -0.017,95% CI:-0.32 至 0.28)。異質性檢定較低且不再顯著( Q = 2.576,df = 2, p = 0.276; I 2 = 22.375)。此分析的森林圖如圖 6所示。
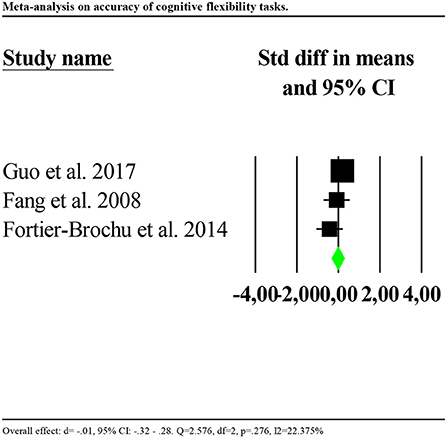
Figure 6. Forest plot of the meta-analysis on accuracy of cognitive flexibility (outlier removed). Results are presented as standardised mean differences (Std diff) and 95% confidence intervals (CI).
圖6 .認知靈活性準確性薈萃分析的森林圖(已刪除異常值)。結果以標準化平均差 (Std diff) 和 95% 信賴區間 (CI) 形式呈現。
In addition, since three studies reported the same outcome using the same task (the number of words produced in the verbal fluency task) (Altena et al., 2008; Siversten et al., 2013; Fortier-Brochu and Morin, 2014), we ran a separate analysis on verbal fluency tasks. Results showed a slight and marginally significant tendency toward a better performance for individuals with insomnia as compared to controls (d = 0.313, 95% CI: −0.000 to 0.617). Heterogeneity tests were low and non-significant (Q = 3.371, df = 2, p = 0.176; I2 = 42.380).
此外,由於三項研究報告了使用相同任務的相同結果(言語流暢性任務中產生的單字數量)( Altena et al., 2008 ; Siversten et al., 2013 ; Fortier-Brochu and Morin, 2014 ),我們對言語流暢性任務進行了單獨的分析。結果顯示,與對照組相比,失眠個體有輕微且略微顯著的表現較好的趨勢( d = 0.313,95% CI:-0.000 至 0.617)。異質性檢定較低且不顯著( Q = 3.371,df = 2, p = 0.176; I 2 = 42.380)。
Risk of Bias 偏見的風險
Risk of bias assessment ratings are reported in Figures 7, 8. In general, studies were judged as having low risk of bias. Small sample size of individual studies emerged as a potential source of bias. Blinding of outcome assessors and participants were judged as two areas of partially biased.
偏倚風險評估評等如圖 7、8所示。一般來說,研究被認為具有較低的偏倚風險。個別研究的小樣本量成為潛在的偏差來源。結果評估者和參與者的盲法被認為是存在部分偏見的兩個領域。
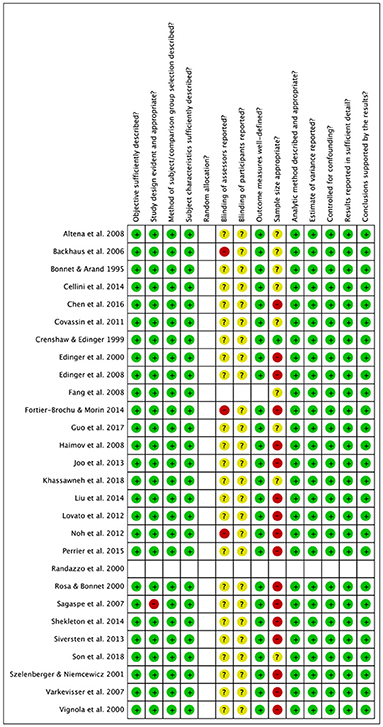
Figure 7. Risk of bias summary.
圖 7 .偏見風險總結。
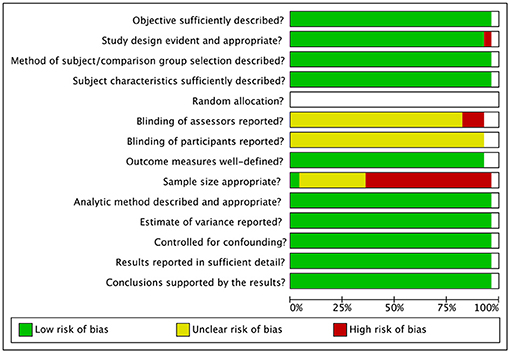
Figure 8. Risk of bias graph.
圖 8 .偏差風險圖。
Discussion 討論
The present systematic review aimed to examine the presence and magnitude of inhibitory control, working memory and cognitive flexibility impairments in individuals with insomnia vs. controls. Using combined narrative synthesis and meta-analysis, we gathered evidence supporting impaired functioning in several aspects of EFs in insomnia. Due to few studies reporting data to compute effect sizes, small sample sizes and high heterogeneity of effects distribution, results from the present review should be interpreted carefully.
本系統性回顧旨在檢視失眠患者與對照組相比,抑制控制、工作記憶和認知靈活性損傷的存在與程度。透過結合敘述綜合和薈萃分析,我們收集了支持失眠中 EF 多個面向功能受損的證據。由於很少有研究報告計算效應量的數據、樣本量小以及效應分佈的高度異質性,因此應仔細解釋本綜述的結果。
Meta-analytic findings support the presence of impaired performance of individuals with insomnia as compared to controls in reaction time-based tasks assessing inhibitory control and cognitive flexibility, with effects sizes ranging from small to moderate in magnitude. In contrast, accuracy rates (i.e., correct responses), were found intact in insomnia with respect to inhibitory control and cognitive flexibility tasks but impaired in working memory tasks. The present work advances knowledge on cognitive functioning in insomnia, updating previous meta-analytic work (Fortier-Brochu et al., 2012) and providing a more detailed assessment of executive processes. In particular, our findings corroborate the results of Fortier-Brochu's review with respect to insomnia-related working memory deficits and provide further evidence for inhibitory control and cognitive flexibility impairments. This advancement is due to the great number of studies (n = 14) published on this topic after Fortier-Brochu's meta-analysis.
統合分析結果支持,在評估抑制控制和認知靈活性的基於反應時間的任務中,與對照組相比,失眠個體存在表現受損的情況,其影響大小從小到中等不等。相較之下,失眠患者在抑制控制和認知靈活性任務方面的準確率(即正確反應)完好無損,但在工作記憶任務方面卻受損。目前的工作推進了有關失眠認知功能的知識,更新了先前的薈萃分析工作( Fortier-Brochu 等人,2012 )並提供了對執行過程的更詳細的評估。特別是,我們的研究結果證實了 Fortier-Brochu 的失眠相關工作記憶缺陷的綜述結果,並為抑制控制和認知靈活性障礙提供了進一步的證據。這項進展歸功於 Fortier-Brochu 的統合分析後就此主題發表的大量研究 ( n = 14)。
Objective Sleep Impairments
客觀睡眠障礙
To examine the hypothesis that EFs are impaired only in insomnia with objective sleep impairments (i.e., shortened TST and/or reduced SE; Fernandez-Mendoza et al., 2010; Vgontzas et al., 2013), which may explain conflicting study findings (Shekleton et al., 2010), we extracted data on the difference between individuals with insomnia and good sleepers on TST and SE. Consequently, we investigated the relationship between presence of EFs impairments and objective sleep impairments. Both narrative synthesis and meta-analysis highlighted that the magnitude of EFs impairments was larger in studies including participants with insomnia and objective shorter TST and/or lower SE as compared to the controls rather than in studies which failed to report significant between group differences in objective sleep or did not report this information. More specifically, this hypothesis was statistically verified for reaction times in inhibitory control tasks and accuracy rates in working memory tasks. Due to the small number of studies, it was not possible to statistically test the objective sleep hypothesis for cognitive flexibility tasks. Nevertheless, these findings could have important implications for treatment development; in particular, tailoring treatment for varying needs, and differential effects of treatment on populations of diverse clinical characteristics.
檢驗 EF 僅在伴隨客觀睡眠障礙的失眠症中受損(即 TST 縮短和/或 SE 降低; Fernandez-Mendoza 等,2010 ; Vgontzas 等,2013 )的假設,這可能解釋相互矛盾的研究結果( Shekleton等人,2010 ),我們提取了失眠者和睡眠良好者在 TST 和 SE 上的差異數據。因此,我們研究了 EF 損傷與客觀睡眠傷害之間的關係。敘述綜合和統合分析都強調,與對照組相比,在包括失眠參與者和客觀較短TST 和/或較低SE 的研究中,EF 損傷的程度更大,而不是在未能報告客觀中組間顯著差異的研究中。更具體地說,這個假設在抑制控制任務的反應時間和工作記憶任務的準確率方面得到了統計驗證。由於研究數量較少,因此無法對認知彈性任務的客觀睡眠假設進行統計檢定。儘管如此,這些發現可能對治療方法的開發產生重要影響;特別是,根據不同的需求量身訂做治療,以及治療對不同臨床特徵族群的不同影響。
These results, therefore, are apparently consistent the hypothesis that higher order neuropsychological functions may be quite preserved in individuals with insomnia with normal sleep and provide partial evidence for the theory that only the phenotype of insomnia with objective sleep impairment is associated with worst objective neuropsychological deficits (Fernandez-Mendoza et al., 2010; Vgontzas et al., 2013). This is also in line with sleep deprivation literature demonstrating an impairment of EFs after sleep loss (Nilsson et al., 2005; Couyoumdjian et al., 2010; Martella et al., 2011).
因此,這些結果顯然與以下假設一致:正常睡眠的失眠個體可能相當保留高級神經心理功能,並為只有客觀睡眠障礙的失眠表型與最嚴重的客觀神經心理缺陷相關的理論提供了部分證據。 ( Fernandez-Mendoza 等人,2010 ; Vgontzas 等人,2013 )。這也與睡眠剝奪文獻一致,證明睡眠不足後 EF 會受損( Nilsson 等人,2005 年; Couyoumdjian 等人,2010 年; Martella 等人,2011 年)。
Nevertheless, due to the small number of studies included in the meta-analytic calculations, these results should be interpreted carefully. Larger trials conducted in both insomnia with normal sleep and objective sleep impairments and including both reaction times and accuracy indices are needed to confirm our findings. Moreover, as discussed in detail below, it is desirable for future studies to elucidate the potentially differential effects of sleep quality and sleep quantity on EFs, that we were unable to investigate due to the small number of studies available.
然而,由於薈萃分析計算中包含的研究數量較少,因此應仔細解釋這些結果。需要對正常睡眠失眠和客觀睡眠障礙進行更大規模的試驗,包括反應時間和準確性指數,以證實我們的發現。此外,如下文詳細討論的,未來的研究需要闡明睡眠品質和睡眠數量對 EF 的潛在差異影響,但由於可用研究數量較少,我們無法對此進行調查。
Cognitive Tests 認知測試
Many neuropsychological tests used to assess EF, such as the trail making test and the Wisconsin card sorting test, have been validated to assess deficits of large magnitude in patients with brain injuries or neurological disorders and are therefore unlikely to detect minor impairment experienced by those without brain injury, such as those with insomnia. Although deficits in the trail making test are reported in samples with severe psychiatric disorder like major depression or bipolar disorder (Pattanayak et al., 2012; Cotrena et al., 2016), other neuropsychological tests such as the colour-word interference tests, backward memory span tasks, and switching attention tasks may be more sensitive to detecting less severe deficits such as those affecting subjects with insomnia. In fact, individuals with insomnia consistently showed impaired performance in these tasks. Thus, future studies of EFs in insomnia samples would benefit from considering for test sensitivity. Importantly, future research on EFs in insomnia would benefit from including tasks with reasonably similar paradigms (i.e., similar instructions and procedure of assessment, similar outcomes). The presence of varied tasks used to assess the same cognitive functions (e.g., 5 different tasks on 13 studies to assess inhibitory control), is a potential source of bias. It would be therefore important for insomnia research to standardise cognitive assessment procedures in order to reduce variability in studies' methodology.
許多用於評估EF 的神經心理學測試,例如追蹤測試和威斯康辛卡片分類測試,已被驗證可以評估腦損傷或神經系統疾病患者的嚴重缺陷,因此不太可能檢測到那些沒有腦損傷或神經系統疾病的患者所經歷的輕微損傷。儘管在患有嚴重憂鬱症或雙相情感障礙等嚴重精神疾病的樣本中報告了線索測試的缺陷( Pattanayak等人,2012年; Cotrena等人,2016年),但其他神經心理學測試,例如色字詞幹擾測試,落後於其他神經心理測驗。事實上,失眠的人在這些任務中表現出一貫的表現受損。因此,未來對失眠樣本中 EF 的研究將受益於考慮測試敏感性。重要的是,未來對失眠 EF 的研究將受益於納入具有相當相似範式的任務(即相似的指導和評估程序、相似的結果)。用於評估相同認知功能的不同任務的存在(例如,13 項研究中的 5 種不同任務來評估抑制控制)是潛在的偏差來源。因此,對於失眠研究來說,標準化認知評估程序以減少研究方法的變異性非常重要。
Age 年齡
A variable that may have potentially influenced the results is age. It has been suggested that different executive processes decline with increasing age, and this decline has been associated with changes in brain areas including frontal lobes and their connections with other brain areas (e.g., Jurado and Rosselli, 2007 for a review). In our sample, about the 60% of the studies reported significant differences between insomnia those with insomnia and controls on EFs, without remarkable differences between studies conducted in adult and elderly populations. Only two studies were conducted on young adults (Covassin et al., 2011; Cellini et al., 2014), and both reported significantly impaired performance in those with insomnia compared to controls respectively on tasks of inhibitory control and working memory. However, the studies were conducted by the same research group and this may potentially limit the generalization of the results. Moreover, differences in age between those with insomnia and controls were limited, with the exception of one study including participants with insomnia 10 years older than controls (Khassawneh et al., 2018). In summary, age is a variable that should be further investigated in cognitive studies conducted in insomnia. Also, there is a dearth of literature on EFs in elderly and young adults with insomnia.
可能影響結果的變數是年齡。有人提出,不同的執行過程會隨著年齡的增長而衰退,這種衰退與大腦區域的變化有關,包括額葉及其與其他大腦區域的連結(例如, Jurado 和 Rosselli,2007 年的綜述)。在我們的樣本中,大約 60% 的研究報告了失眠患者與 EF 對照組之間存在顯著差異,但在成人和老年人群中進行的研究之間沒有顯著差異。僅對年輕人進行了兩項研究( Covassin 等人,2011 年; Cellini 等人,2014 年),兩項研究均報告,與對照組相比,失眠者在抑制控制和工作記憶任務方面的表現明顯受損。然而,這些研究是由同一研究小組進行的,這可能會限制結果的推廣。此外,失眠患者和對照組之間的年齡差異有限,但一項研究除外,其中失眠參與者比對照組大 10 歲( Khassawneh 等人,2018 )。總之,年齡是一個在失眠認知研究中應該進一步研究的變項。此外,關於老年人和年輕人失眠的 EF 的文獻也很少。
Limitations 限制
Although the current review provides a comprehensive synthesis of the literature concerning EFs and insomnia, there are several limitations which should be acknowledged. Consistent with Cochrane guidelines for systematic reviews (Higgins and Green, 2011), we searched three databases. It is possible that searching additional databases (e.g., EMBASE) may have produced additional studies, although our other approaches (e.g., searching reference lists of included papers) make this less likely. Also, in this review, we adopted the definition of EFs based on inhibitory control, working memory, and cognitive flexibility (Miyake et al., 2000; Diamond, 2013), a very influential classification recently used in the context of insomnia research (Fernandez-Mendoza et al., 2010; Vgontzas et al., 2013). However, as aforementioned, controversies and divergences on the definition and conceptualisation of EFs, with many other models of EFs previously proposed (see Gratton et al., 2017 for a review); thus, future systematic reviews integrating those models may highlight further important findings and achieve different conclusions. Additionally, the identification and categorisation of executive tasks used in this review may also present some limitations. We decided to base the identification and categorisation of the tests on recent literature (Fortier-Brochu et al., 2012; Diamond, 2013; Snyder et al., 2015) whilst other researchers in the field have used different classifications (Shekleton et al., 2010). Thus, it is possible that slightly different results may emerge due to the use of different classifications of the tasks. Also, we decided to extract data on objective sleep derived from both actigraphy and polysomnography and to consider these measures in the same analysis. Although both measures allow to objectively assess TST and SE, the two measures are based on different psychophysiological processes. Actigraphy is based on body movements while polysomnography is based on a combination of electroencephalogram, electrooculogram and electromyogram, which also permits derivation of sleep architecture information. It has been observed in validation studies, that TST and SE derived from the two methods of assessment correlate (r = 0.87 for TST and r = 0.56 for SE; e.g., Lichstein et al., 2006; Williams et al., 2018). However, contrasting evidence also suggested limited validity of actigraphy when compared to polysomnography (e.g., Sànchez-Ortun o et al., 2010; Natale et al., 2014). We decided to pool them in the same analysis to reach a sufficient number of effect sizes to analyse. However, given contrasting literature, the two measures may be ideally considered in different analyses in future studies with larger samples. Relatedly, we focussed on TST and SE as two measures reflecting night-time symptoms of insomnia (i.e., longer time needed to fall asleep, frequent and long nocturnal awakenings). While TST is a measure of sleep duration, SE is generally considered a measure of general sleep quality. Thus, the two measures may potentially have differential effects on EFs. Given the limited number of studies included in this review, we were limited in investigating the differential effect of SE and TST on EFs in meta-analysis. Again, it is important for future studies to include objective measures of SE and TST to better elucidate their effects on EFs performance in insomnia.
儘管目前的綜述對 EF 和失眠的文獻進行了全面綜合,但仍存在一些應承認的限制。根據 Cochrane 系統性回顧指南( Higgins 和 Green,2011 ),我們檢索了三個資料庫。搜尋其他資料庫(例如,EMBASE)可能會產生額外的研究,儘管我們的其他方法(例如,搜尋所包含論文的參考文獻清單)使這種可能性較小。此外,在這篇綜述中,我們採用了基於抑制控制、工作記憶和認知靈活性的 EF 定義( Miyake 等人,2000 年; Diamond,2013 年),這是最近在失眠研究中使用的一個非常有影響力的分類( Fernandez ) -Mendoza 等人,2010 ; Vgontzas 等人,2013 )。然而,如上所述,EF 的定義和概念化存在爭議和分歧,先前提出了許多其他 EF 模型(參見Gratton 等人,2017 年綜述);因此,未來整合這些模型的系統性回顧可能會突顯進一步的重要發現並得出不同的結論。此外,本次審查中所使用的執行任務的識別和分類也可能存在一些限制。我們決定根據最近的文獻對測試進行識別和分類( Fortier-Brochu 等人,2012 年; Diamond,2013 年; Snyder 等人,2015 年),而該領域的其他研究人員使用了不同的分類( Shekleton 等人,2015 年) 。因此,由於使用不同的任務分類,可能會出現略有不同的結果。 此外,我們決定從體動記錄器和多導睡眠圖中提取客觀睡眠數據,並在同一分析中考慮這些措施。儘管這兩種測量方法都可以客觀地評估 TST 和 SE,但這兩種測量方法是基於不同的心理生理過程。體動記錄器是基於身體運動,而多導睡眠圖則是基於腦電圖、眼電圖和肌電圖的組合,這也可以導出睡眠結構資訊。在驗證研究中觀察到,兩種評估方法得出的 TST 和 SE 具有相關性(TST 的r = 0.87,SE 的r = 0.56;例如, Lichstein 等人,2006 年; Williams 等人,2018 年)。然而,對比證據也表明,與多導睡眠圖相比,體動記錄器的有效性有限(例如, Sànchez-Ortun o 等人,2010 ; Natale 等人,2014 )。我們決定將它們集中在同一分析中,以達到足夠數量的效應大小進行分析。然而,鑑於文獻對比,在未來更大樣本的研究中,理想情況下可以在不同的分析中考慮這兩種措施。與此相關,我們將 TST 和 SE 作為反映夜間失眠症狀(即入睡時間較長、夜間頻繁醒來)的兩個指標。 TST 是睡眠時間的衡量標準,而 SE 通常被認為是一般睡眠品質的衡量標準。因此,這兩種措施可能對 EF 產生不同的影響。鑑於本綜述中納入的研究數量有限,我們在統合分析中研究 SE 和 TST 對 EF 的差異影響的能力有限。 同樣,未來的研究重要的是包括 SE 和 TST 的客觀測量,以更好地闡明它們對失眠中 EF 表現的影響。
Conclusions 結論
The study of EFs has dramatically increased in recent years in the context of mental health. However, EFs are still under-investigated in insomnia. To make a comparison, a recent and already cited review of meta-analytic literature (Snyder et al., 2015) found that ten meta-analyses were conducted studying EFs in bipolar, eight in schizophrenia, seven in substance use, four in anxiety and two in depressive disorders, while only one meta-analysis was conducted in samples with insomnia (Fortier-Brochu et al., 2012). This discrepancy is particularly surprising given the well documented detrimental effects of insomnia on daytime variables in which EFs may play an important role, such as memory, attention and concentration and emotion regulation (Kyle et al., 2013; Harris et al., 2015; Cellini, 2016) and the consideration of insomnia as a transdiagnostic process across mental disorders (Harvey, 2009; Dolsen et al., 2014). Future studies with comparable procedures of neuropsychological assessment are needed to clarify the nature and strength of the association between insomnia and EFs deficits. Such standardisation of assessments could lead to important clinical and research applications. Interventional studies, aiming at investigating whether EFs impairments in insomnia are reversible are needed. Randomised controlled trials of cognitive behavioural therapy for insomnia showed promising results on core EFs (Herbert et al., 2018). Nevertheless, replication studies are needed to consolidate these results and evaluate the cost-effectiveness of such treatment approaches on factors including healthcare utilisation and burden of illness (e.g., absenteeism, workplace errors, quality of life). Additionally, it is yet to be explored whether improvement in EFs after insomnia treatment is associated with ameliorate subjective functioning (Kyle et al., 2013; Ballesio et al., 2018). Future research is particularly needed on elderly and young adults which are under-investigated populations. Moreover, researchers should consider variables that are largely neglected in this field, including, besides objective sleep, the time of testing, that may influence study results due the fluctuations of circadian rhythm (e.g., Varkevisser and Kerkhof, 2005).
近年來,在心理健康方面對 EF 的研究急劇增加。然而,EF 在失眠方面的研究仍不足。為了進行比較,最近一篇已引用的統合分析文獻綜述( Snyder 等,2015 )發現,進行了10 項統合分析,研究雙相情感障礙、8 項精神分裂症、7 項物質使用、4 項焦慮症和兩項針對憂鬱症樣本,而僅對失眠樣本進行了一項薈萃分析( Fortier-Brochu 等,2012 )。這種差異尤其令人驚訝,因為有充分記錄的失眠對白天變數的有害影響,其中 EF 可能發揮重要作用,例如記憶、注意力和注意力以及情緒調節( Kyle 等人,2013 年; Harris 等人,2015 年; Cellini,2016 )以及將失眠視為精神障礙的跨診斷過程( Harvey,2009 ; Dolsen 等,2014 )。未來需要進行類似的神經心理學評估程序的研究,以闡明失眠與 EF 缺陷之間關聯的性質和強度。這種評估標準化可能會帶來重要的臨床和研究應用。需要進行幹預性研究,旨在調查失眠引起的 EF 損傷是否可逆。失眠認知行為療法的隨機對照試驗在核心 EF 方面顯示出有希望的結果( Herbert 等人,2018 )。然而,需要進行重複研究來鞏固這些結果,並根據醫療保健利用和疾病負擔等因素評估此類治療方法的成本效益(例如、缺勤、工作場所錯誤、生活品質)。此外,還有待探討失眠治療後 EF 的改善是否與主觀功能的改善有關( Kyle 等,2013 ; Ballesio 等,2018 )。未來的研究尤其需要針對尚未充分調查的老年人和年輕人。此外,研究人員應該考慮該領域很大程度上被忽視的變量,除了客觀睡眠之外,還包括測試時間,這些變量可能因晝夜節律的波動而影響研究結果(例如, Varkevisser和Kerkhof,2005 )。
Author Contributions 作者貢獻
AB run the literature searches, extracted qualitative and quantitative data, assessed the risk of bias, run the analyses, and wrote the draft of the manuscript. MRJVA screened the abstracts and full-texts, assessed the risk of bias, and revised the draft. SK, FF, and CL provided intellectual and analytical advices, supervised the work, and revised the manuscript.
AB 進行文獻檢索、擷取定性和定量資料、評估偏倚風險、進行分析並撰寫稿件草稿。 MRJVA 篩選了摘要和全文,評估了偏倚風險,並對草案進行了修改。 SK、FF 和 CL 提供了知識和分析建議、監督工作並修改了手稿。
Conflict of Interest Statement
利益衝突聲明
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
作者聲明,該研究是在不存在任何可能被視為潛在利益衝突的商業或財務關係的情況下進行的。
Supplementary Material 補充資料
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyg.2019.00101/full#supplementary-material
本文的補充資料可在線找到: https://www.frontiersin.org/articles/10.3389/fpsyg.2019.00101/full#supplementary-material
References 參考
Altena, E., Van Der Werf, Y. D., Sanz-Arigita, E. J., Voorn, T. A., Rombouts, S. A. R. B., Kuijer, J. P. A., et al. (2008). Prefrontal hypoactivation and recovery in insomnia. Sleep 31, 1271–1276. doi: 10.5665/sleep/31.9.1271
Altena, E.、Van Der Werf, YD、Sanz-Arigita, EJ、Voorn, TA、Rombouts、SARB、Kuijer, JPA 等。 (2008)。失眠中的前額葉活化不足和恢復。睡眠31, 1271–1276。 doi:10.5665/睡眠/31.9.1271
PubMed Abstract | CrossRef Full Text | Google Scholar
考研摘要|全文交叉引用|谷歌學術
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Washington, DC: American Psychiatric Association.
美國精神醫學會(2013)。精神疾病診斷與統計手冊:DSM-5 。華盛頓特區:美國精神病學協會。
Aron, A. R., Robbins, T. W., and Poldrack, R. A. (2004). Inhibition and the right inferior frontal cortex. Trends. Cogn. Sci. 8, 170–177. doi: 10.1016/j.tics.2004.02.010
阿倫 (AR)、羅賓斯 (TW) 和波德拉克 (RA) (2004)。抑制與右額下皮質。趨勢。認知。科學。 8、170-177。 doi:10.1016/j.tics.2004.02.010
PubMed Abstract | CrossRef Full Text | Google Scholar
考研摘要|全文交叉引用|谷歌學術
Backhaus, J., Junghanns, K., Born, J., Hohaus, K., Faasch, F., and Hohagen, F. (2006). Impaired declarative memory consolidation during sleep in patients with primary insomnia: influence of sleep architecture and nocturnal cortisol release. Bio. Psychiatry 60, 1324–1330. doi: 10.1016/j.biopsych.2006.03.051
Backhaus, J.、Junghanns, K.、Born, J.、Hohaus, K.、Faasch, F. 與 Hohagen, F. (2006)。原發性失眠患者在睡眠期間陳述性記憶鞏固受損:睡眠結構和夜間皮質醇釋放的影響。生物。精神病學60, 1324–1330。 doi:10.1016/j.biopsych.2006.03.051
PubMed Abstract | CrossRef Full Text | Google Scholar
考研摘要|全文交叉引用|谷歌學術
Ballesio, A., Ottaviani, C., and Lombardo, C (2018). Poor cognitive inhibition predicts rumination about insomnia in a clinical sample. Behav. Sleep Med. 2018, 1–10. doi: 10.1080/15402002.2018.1461103
Ballesio, A.、Ottaviani, C. 與 Lombardo, C (2018)。不良的認知抑制預示著臨床樣本中對失眠的沉思。行為。睡眠醫學。 2018 年,1-10。號碼:10.1080/15402002.2018.1461103
Bonnet, M. H., and Arand, D. L. (1995). 24-hour metabolic rate in insomniacs and matched nocturnal sleepers. Sleep 18, 581–588. doi: 10.1093/sleep/18.7.581
Bonnet, MH 與 Arand, DL (1995)。失眠症患者和夜間睡眠者的 24 小時代謝率。睡眠18,581–588。 doi:10.1093/睡眠/18.7.581
Calem, M., Bisla, J., Dewey, M., Bebbington, P. E., Brugha, T., Cooper, C., et al. (2012). Increased prevalence of insomnia and changes in hypnotics use in England over 15 years: analysis of the 1993, 2000, and 2007 National Psychiatric Morbidity Surveys. Sleep 35, 377–384. doi: 10.5665/sleep.1700
Calem, M.、Bisla, J.、Dewey, M.、Bebbington, PE、Brugha, T.、Cooper, C. 等。 (2012)。 15 年來英國失眠盛行率的增加和安眠藥使用的變化:對 1993 年、2000 年和 2007 年國家精神病學發病率調查的分析。睡眠35, 377–384。 doi: 10.5665/sleep.1700
PubMed Abstract | CrossRef Full Text | Google Scholar
考研摘要|全文交叉引用|谷歌學術
Carney, C., Buysse, D. J., Ancoli-Israeli, S., Edinger, K. D., Krystal, K. D., Lichstein, K. L., et al. (2012). The Consensus Sleep Diary: standardizing prospective sleep self-monitoring. Sleep 35, 287–302. doi: 10.5665/sleep.1642
Carney, C.、Buysse, DJ、Ancoli-Israeli, S.、Edinger, KD、Krystal, KD、Lichstein, KL 等。 (2012)。共識睡眠日記:標準化前瞻性睡眠自我監測。睡眠35, 287–302。 doi:10.5665/sleep.1642
PubMed Abstract | CrossRef Full Text | Google Scholar
考研摘要|全文交叉引用|谷歌學術
Cellini, N. (2016). Memory consolidation in sleep disorders. Sleep Med. Rev. 35, 101–112. doi: 10.1016/j.smrv.2016.09.003
切利尼,N.(2016)。睡眠障礙中的記憶鞏固。睡眠醫學。牧師。 35、101-112。 DOI:10.1016/j.smrv.2016.09.003
PubMed Abstract | CrossRef Full Text | Google Scholar
考研摘要|全文交叉引用|谷歌學術
Cellini, N., de Zambotti, M., Covassin, N., Sarlo, M., and Stegagno, L. (2014). Working memory impairment and cardiovascular hyperarousal in young primary insomniacs. Psychophysiology 51, 206–214. doi: 10.1111/psyp.12167
Cellini, N.、de Zambotti, M.、Covassin, N.、Sarlo, M. 與 Stegagno, L. (2014)。年輕原發性失眠症患者的工作記憶障礙與心血管過度覺醒。心理生理學51, 206–214。 doi:10.1111/psyp.12167
PubMed Abstract | CrossRef Full Text | Google Scholar
考研摘要|全文交叉引用|谷歌學術
Chaput, J. P., Yau, J., Rao, D. P., and Morin, C. M. (2018). Prevalence of insomnia for Canadians aged 6 to 79. Health Rep. 29, 16–20.
Chaput, JP、Yau, J.、Rao, DP 與 Morin, CM (2018)。 6 至 79 歲加拿大人的失眠盛行率。 29、16-20。
Chen, G. H., Xia, L., Wang, F., Li, X. W., and Jiao, C. A. (2016). Patients with chronic insomnia have selective impairments in memory that are modulated by cortisol. Psychophysiol 53, 1567–1576. doi: 10.1111/psyp.12700
Chen, GH、Xia, L.、Wang, F.、Li, XW 與 Jiao, CA (2016)。慢性失眠患者的記憶力會受到皮質醇的調節而出現選擇性損傷。心理生理學53, 1567–1576。 doi:10.1111/psyp.12700
PubMed Abstract | CrossRef Full Text | Google Scholar
考研摘要|全文交叉引用|谷歌學術
Cotrena, C., Branco, L. D., Shansis, F. M., and Fonseca, R. P. (2016). Executive function impairments in depression and bipolar disorder: association with functional impairment and quality of life. J. Affect. Disord. 190, 744–753. doi: 10.1016/j.jad.2015.11.007
Cotrena, C.、Branco, LD、Shansis, FM 和 Fonseca, RP (2016)。憂鬱症和躁鬱症的執行功能障礙:與功能障礙和生活品質的關聯。 J.影響。混亂。 190、744–753。 doi:10.1016/j.jad.2015.11.007
PubMed Abstract | CrossRef Full Text | Google Scholar
考研摘要|全文交叉引用|谷歌學術
Couyoumdjian, A., Sdoia, S., Tempesta, D., Curcio, G., Rastellini, E., De Gennaro, L., et al. (2010). The effects of sleep and sleep deprivation on task-switching performance. J. Sleep Res. 19(1Pt 1), 64–70. doi: 10.1111/j.1365-2869.2009.00774.x
Couyoumdjian, A.、Sdoia, S.、Tempesta, D.、Curcio, G.、Rastellini, E.、De Gennaro, L. 等。 (2010)。睡眠和睡眠剝奪對任務切換表現的影響。 J.睡眠研究。 19(1 第 1 部分),64–70。 doi:10.1111/j.1365-2869.2009.00774.x
PubMed Abstract | CrossRef Full Text | Google Scholar
考研摘要|全文交叉引用|谷歌學術
Covassin, N., de Zambotti, M., Sarlo, M., De Min Tona, G., Sarasso, S., and Stegagno, L. (2011). Cognitive performance and cardiovascular markers of hyperarousal in primary insomnia. Int. J. Psychophysiol. 80, 76–86. doi: 10.1016/j.ijpsycho.2011.02.005
Covassin, N.、de Zambotti, M.、Sarlo, M.、De Min Tona, G.、Sarasso, S. 與 Stegagno, L. (2011)。原發性失眠中過度覺醒的認知表現和心血管標記。國際。 J.心理生理學。 80、76–86。 doi:10.1016/j.ijpsycho.2011.02.005
PubMed Abstract | CrossRef Full Text | Google Scholar
考研摘要|全文交叉引用|谷歌學術
Crenshaw, M. C., and Edinger, J. D. (1999). Slow-wave sleep and waking performance among older adults with and without insomnia complaints. Physiol. Behav. 66, 485–492. doi: 10.1016/S0031-9384(98)00316-3
Diamond, A. (2013). Executive functions. Annu. Rev. Psychol. 64:135–168. doi: 10.1146/annurev-psych-113011-143750
Dolsen, M. R., Asarnow, L. D., and Harvey, A. G. (2014). Insomnia as transdiagnostic process in psychiatric disorders. Curr. Psychiatry Rep. 16:471. doi: 10.1007/s11920-014-0471-y
Duncan, J. (2010). The multiple-demand (MD) system of the primate brain: mental programs for intelligent behaviour. Trends Cogn. Sci. 14, 172–179. doi: 10.1016/j.tics.2010.01.004
Edinger, J. D., Glenn, D. M., Bastian, L. A., and Marsh, G. R. (2000). Slow-wave sleep and waking cognitive performance II: findings among middle-aged adults with and without insomnia complaints. Physiol. Behav. 70, 127–134. doi: 10.1016/S0031-9384(00)00238-9
Edinger, J. D., Means, M. K., Carney, C. E., and Krystal, A. D. (2008). Psychomotor performance deficits and their relation to prior nights' sleep among individuals with primary insomnia. Sleep 31, 599–607. doi: 10.1093/sleep/31.5.599
Espie, C. A., Broomfield, N. M., MacMahon, K. M., Macphee, L. M., and Taylor, L. M. (2006). The attention-intention-effort pathway in the development of psychophysiological insomnia: a theoretical review. Sleep Med. Rev. 10, 215–245. doi: 10.1016/j.smrv.2006.03.002
Fang, S. C., Huang, C. J., Yang, T. T., and Tsai, P. S. (2008). Heart rate variability and daytime functioning in insomniacs and normal sleepers: preliminary results. J. Psychosom. Res. 65, 23–30. doi: 10.1016/j.jpsychores.2008.02.003
Fernandez-Mendoza, J., Calhoun, S., Bixler, E. O., Pejovic, S., Karataraki, M., Liao, D., et al. (2010). Insomnia with objective short sleep duration is associated with deficits in neuropsychological performance: a general population study. Sleep 33, 459–465. doi: 10.1093/sleep/33.4.459
Fortier-Brochu, E., Beaulieu-Bonneau, S., Ivers, H., and Morin, C. M. (2012). Insomnia and daytime cognitive impairments: a meta-analysis. Sleep Med. Rev. 16, 83–94. doi: 10.1016/j.smrv.2011.03.008
Fortier-Brochu, E., and Morin, C. M. (2014). Cognitive impairment in individuals with insomnia: clinical significance and correlates. Sleep 37, 1787–1798. doi: 10.5665/sleep.4172
Gratton, G., Cooper, P., Fabiani, M., Carter, C. S., and Karayanidis, F. (2017). Dynamics of cognitive control: theoretical bases, paradigms, and a view for the future. Psychophysiol 55:e13016. doi: 10.1111/psyp.13016
Guo, H., Wei, M., and Ding, W. (2017). Changes in cognitive function in patients with primary insomnia. Shanghai Arch. Psychiatry 29, 137–145. doi: 10.11919/j.issn.1002-0829.216097
Gustavsson, A., Svensson, M., Jacobi, F., Allgulander, C., Alonso, G., Beghi, E., et al. (2011). Cost of disorders of the brain in Europe 2010. Eur. Neuropsychopharmacol. 2, 655–679. doi: 10.1016/j.euroneuro.2011.08.008
Haimov, I., Hanuka, E., and Horowitz, Y. (2008). Chronic insomnia and cognitive functioning among older adults. Behav. Sleep Med. 6, 32–54. doi: 10.1080/15402000701796080
Harris, K., Spiegelhalder, K., Espie, C. A., MacMahon, K. M., Woods, H. C., and Kyle, S. D. (2015). Sleep-related attentional bias in insomnia: state of the science review. Clin. Psychol. Rev. 42, 16–27. doi: 10.1016/j.cpr.2015.08.001
Harvey, A. G. (2002). Cognitive model of insomnia. Behav. Res. Ther. 40, 869–893. doi: 10.1016/S0005-7967(01)00061-4
Harvey, A. G. (2009). A transdiagnostic approach to treating sleep disturbance in psychiatric disorders. Cogn. Behav. Ther. 38(Suppl. 1), 35–42. doi: 10.1080/16506070903033825
Herbert, V., Kyle, S. D., and Pratt, D. (2018). Does cognitive behavioural therapy for insomnia improve cognitive performance? A systematic review and narrative synthesis. Sleep. Med. Rev. 39, 37–51. doi: 10.1016/j.smrv.2017.07.001
Higgins, J. P. T., and Green, S. (eds.). (2011). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration.
Joo, E. Y., Noh, H. J., Kim, J. S., Koo, D. L., Kim, D., Hwang, K. J., et al. (2013). Brain gray matter deficits in patients with chronic primary insomnia. Sleep 36, 999–1007. doi: 10.5665/sleep.2796
Jurado, M. B., and Rosselli, M. (2007). The elusive nature of executive functions: a review of our current understanding. Neuropsychol. Rev. 17, 213–233. doi: 10.1007/s11065-007-9040-z
Khassawneh, B. Y., Bathgate, C. J., Tsai, S. C., and Edinger, J. D. (2018). Neurocognitive performance in insomnia disorder: the impact of hyperarousal and short sleep duration. J. Sleep Res. 2018:e12747. doi: 10.1111/jsr.12747
Killgore, W. D., Kahn-Greene, E. T., Grugle, N. L., Killgore, D. B., and Balkin, T. J. (2009). Sustaining executive functions during sleep deprivation: a comparison of caffeine, dextroamphetamine, and modafinil. Sleep 32, 205–216. doi: 10.1093/sleep/32.2.205
Killgore, W. D., Kamimori, G. H., and Balkin, T. J. (2014). Caffeine improves the efficiency of planning and sequencing abilities during sleep deprivation. J. Clin. Psychopharmacol. 34, 660–662. doi: 10.1097/JCP.0000000000000184
Kmet, L. M., Lee, R. C., and Cook, L. S. (2004). Standard Quality Assessment Criteria for Evaluating Primary Research Papers From a Variety of Fields. Edmonton: Alberta Heritage Foundation for Medical Research (AHFMR). HTA Initiative #13.
Kyle, S. D., Crawford, M. R., Morgan, K., Spiegelhalder, K., Clark, A. A., and Espie, C. A. (2013). The Glasgow Sleep Impact Index (GSII): a novel patient-centred measure for assessing sleep-related quality of life impairment in Insomnia Disorder. Sleep Med. 14, 493–501. doi: 10.1016/j.sleep.2012.10.023
Lichstein, K. L., Stone, K. C., Donaldson, J., Nau, S. D., Soeffing, J. P., Murray, D., et al. (2006). Actigraphy validation in insomnia. Sleep 29, 232–239. doi: 10.1093/sleep/29.2.232
Liu, H., Wang, D., Li, Y., Li, Z., Zhang, Y., Lei, F., et al. (2014). Examination of daytime sleepiness and cognitive performance testing in patients with primary insomnia. PLoS ONE 9:e100965. doi: 10.1371/journal.pone.0100965
Lovato, N., Lack, L., Wright, H., Cant, M., and Humphreys, J. (2013). Working memory performance of older adults with insomnia. J. Sleep Res. 22, 251–257. doi: 10.1111/jsr.12010
Martella, D., Casagrande, M., and Lupiáñez, J. (2011). Alerting, orienting and executive control: the effects of sleep deprivation on attentional networks. Exp. Brain. Res. 210, 81–89. doi: 10.1007/s00221-011-2605-3
Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., and Wager, T. D. (2000). The unity and diversity of executive functions and their contributions to complex “frontal lobe” tasks: a latent variable analysis. Cogn. Psychol. 41, 49–100. doi: 10.1006/cogp.1999.0734
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D. G. (2009). The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann. Intern. Med. 151, 264–269. doi: 10.7326/0003-4819-151-4-200908180-00135
Natale, V., Lèger, D., Martoni, M., Bayon, V., and Erbacci, A. (2014). The role of actigraphy in the assessment of primary insomnia: a retrospective study. Sleep Med. 15, 111–115. doi: 10.1016/j.sleep.2013.08.792
Nilsson, J. P., Söderström, M., Karlsson, A. U., Lekander, M., Akerstedt, T., Lindroth, N. E., et al. (2005). Less effective executive functioning after a night of sleep deprivation. J. Sleep. Res. 14, 1–6. doi: 10.1111/j.1365-2869.2005.00442.x
Noh, H. J., Joo, E. Y., Kim, S. T., Yoon, D. L., Kim, D., Lee, G. H., et al. (2012). The relationship between hippocampal volume and cognition in patients with chronic primary insomnia. J. Clin. Neurol. 8, 130–138. doi: 10.3988/jcn.2012.8.2.130
Nowrangi, M. A., Lyketsos, C., Rao, V., and Munro, C. A. (2014). Systematic review of neuroimaging correlates of executive functioning: converging evidence from different clinical populations. J. Neuropsychiatry Clin. Neurosci. 26, 114–125. doi: 10.1176/appi.neuropsych.12070176
Pattanayak, R. D., Sagar, R., and Mehta, M. (2012). Neuropsychological performance in euthymic Indian patients with bipolar disorder type I: correlation between quality of life and global functioning. Psychiatry Clin. Neurosci. 66, 553–563. doi: 10.1111/j.1440-1819.2012.02400.x
Perlis, M. L., Giles, D. E., Mendelson, W. B., Bootzin, R. R., and Wyatt, J. K. (1997). Psychophysiological insomnia: the behavioral model and neurocognitive perspective. J. Sleep Res. 6, 179–188. doi: 10.1046/j.1365-2869.1997.00045.x
Perrier, J., Chavoix, C., and Bocca, M. L. (2015). Functioning of the three attentional networks in primary insomnia. Sleep Med. 16, 1569–1575. doi: 10.1016/j.sleep.2015.06.025
Popay, J., Roberts, H., Sowden, A., Petticrew, M., Arrai, L., Rodgers, M., et al. (2006). Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A Product From the ESRC Methods Programme. Lancaster University.
Randazzo, A. C., Schweitzer, P. K., Stone, K. L., Compton, J. D., and Walsh, J. K. (2000). Impaired cognitive function in insomniacs vs. normals. Sleep 23(Suppl.):A4.
Repovs, G., and Baddeley, A. (2006). The multi-component model of working memory: explorations in experimental cognitive psychology. Neuroscience 139, 5–21. doi: 10.1016/j.neuroscience.2005.12.061
Rosa, R. R., and Bonnet, M. H. (2000). Reported chronic insomnia is independent of poor sleep as measured by electroencephalography. Psychosom. Med. 62, 474–482. doi: 10.1097/00006842-200007000-00004
Sagaspe, P., Philip, P., and Schwartz, S. (2007). Inhibitory motor control in apneic and insomniac patients: a stop task study. J. Sleep Res. 16, 381–387. doi: 10.1111/j.1365-2869.2007.00607.x
Sànchez-Ortun o, M. M., Edinger, J. D., Means, M. K., and Almirall, D. (2010). Home is where sleep is: an ecological approach to test the validity of actigraphy for the assessment of insomnia. Sleep 6, 21–29.
Schmidt, R. E., Richter, M., Gendolla, G. H., and Van der Linden, M. (2014). Young poor sleepers mobilize extra effort in an easy memory task: evidence from cardiovascular measures. J. Sleep. Res. 19, 487–495. doi: 10.1111/j.1365-2869.2010.00834.x
Shekleton, J. A., Flynn-Evans, E. E., Miller, B., Epstein, L. J., Kirsch, D., Brogna, A., et al. (2014). Neurobehavioral performance impairment in insomnia: relationship with self-reported sleep and daytime functioning. Sleep 37, 107–116. doi: 10.5665/sleep.3318
Shekleton, J. A., Rogers, N. L., and Rajaratnam, S. M. (2010). Searching for the daytime impairments of primary insomnia. Sleep Med. Rev. 14, 47–60. doi: 10.1016/j.smrv.2009.06.001
Siversten, B., Hysing, M., Wehling, E., Pallesen, S., Nordhus, I. H., Espeseth, T., et al. (2013). Neuropsychological performance in older insomniacs. Aging. Neuropsychol. Dev. Cogn. 20, 34–48. doi: 10.1080/13825585.2012.672947
Snyder, H. R., Miyake, A., and Hankin, B. L. (2015). Advancing understanding of executive function impairments and psychopathology: bridging the gap between clinical and cognitive approaches. Front. Psychol. 6:328. doi: 10.3389/fpsyg.2015.00328
Son, Y. D., Kang, J. M., Cho, S. J., Lee, J. S., Hwang, H. Y., and Kang, S. G. (2018). fMRI brain activation in patients with insomnia disorder during a working memory task. Sleep Breath 22:487493. doi: 10.1007/s11325-017-1575-5
Szelenberger, W., and Niemcewicz, S. (2001). Event-related current density in primary insomnia. Acta Neurobiol. Exp. 61, 299–308.
Varkevisser, M., and Kerkhof, G. A. (2005). Chronic insomnia and performance in a 25h constant routine study. J. Sleep. Res. 14, 49–59. doi: 10.1111/j.1365-2869.2004.00414.x
Varkevisser, M., Van Dongen, H. P., Kerkhof, G. A., and van Amsterdam, J. (2007). Chronic insomnia and ambulatory daytime functioning. Behav. Sleep. Med. 5, 279–296. doi: 10.1080/15402000701557425
Vaughan, L., and Giovanello, K. (2010). Executive function in daily life: Age-related influences of executive processes on instrumental activities of daily living. Psychol. Aging 25, 343–355. doi: 10.1037/a0017729
Vgontzas, A. N., Fernandez-Mendoza, J., Liao, D., and Bixler, E. O. (2013). Insomnia with objective short sleep duration: the most biologically severe phenotype of the disorder. Sleep Med. Rev. 17, 241–254. doi: 10.1016/j.smrv.2012.09.005
Vignola, A., Lamoureux, C., Bastien, C. H., and Morin, C. M. (2000). Effects of chronic insomnia and use of benzodiazepines on daytime performance in older adults. J. Gerontol. 55, 54–62. doi: 10.1093/geronb/55.1.P54
Williams, J. M., Taylor, D. J., Slavish, D. C., Gardner, C. E., Zimmerman, M. R., Patel, K., et al. (2018). Validity of actigraphy in young adults with insomnia. Behav. Sleep. Med. 25, 1–16. doi: 10.1080/15402002.2018.1545653
Yang, Y., Cao, S., Shields, G. S., Teng, Z., and Liu, Y. (2016). The relationship between rumination and core executive functions: a meta-analysis. Depress. Anxiety 34, 37–50. doi: 10.1002/da.22539
Keywords: insomnia, executive functions, inhibition, working memory, flexibility, prefrontal cortex, cognition
Citation: Ballesio A, Aquino MRJV, Kyle SD, Ferlazzo F and Lombardo C (2019) Executive Functions in Insomnia Disorder: A Systematic Review and Exploratory Meta-Analysis. Front. Psychol. 10:101. doi: 10.3389/fpsyg.2019.00101
Received: 24 October 2018; Accepted: 14 January 2019;
Published: 30 January 2019.
Edited by:
Kathrin Finke, Friedrich-Schiller-Universität Jena, GermanyReviewed by:
Katie Moraes de Almondes, Federal University of Rio Grande do Norte, BrazilJoy Perrier, INSERM U1077 Neuropsychologie et Imagerie de la Mémoire Humaine, France
Copyright © 2019 Ballesio, Aquino, Kyle, Ferlazzo and Lombardo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea Ballesio, andrea.ballesio@uniroma1.it